Van Matre Edward T, Mueller Scott W, Fish Douglas N, MacLaren Robert, Cava Luis F, Neumann Robert T, Kiser Tyree H
Department of Clinical Pharmacy, University of Colorado Skaggs School of Pharmacy and Pharmaceutical Sciences, Aurora, CO, USA.
Department of Neurosurgery, University of Colorado School of Medicine, Aurora, CO, USA.
Am J Case Rep. 2017 Apr 27;18:458-462. doi: 10.12659/ajcr.902709.
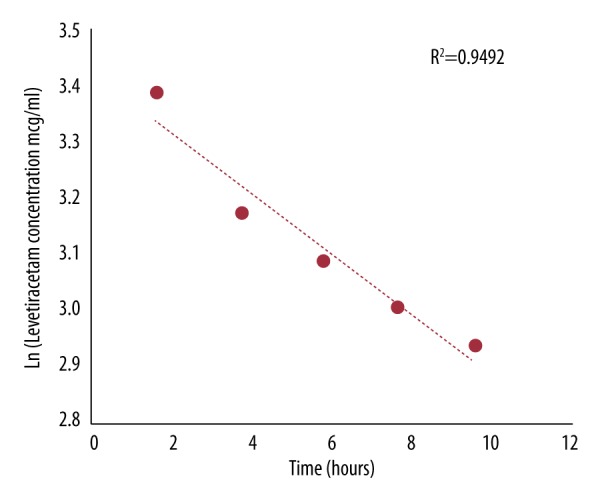
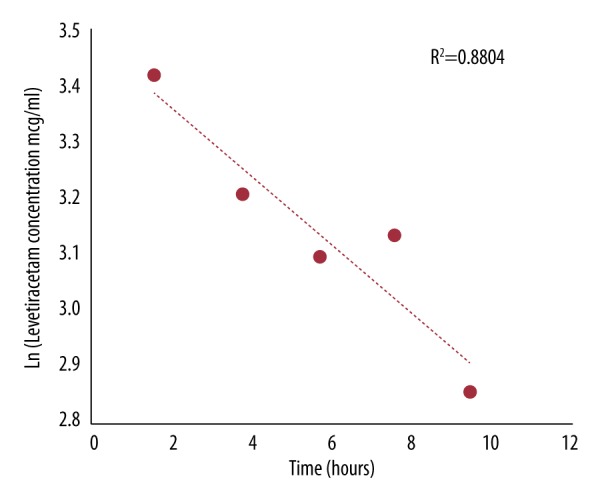
BACKGROUND Levetiracetam is an antiepileptic drug frequently used in critically ill patients. Levetiracetam is primarily eliminated as a parent compound via glomerular filtration and requires dose adjustment in renal insufficiency, but the literature on patients receiving continuous veno-venous hemofiltration (CVVH) is scant. CASE REPORT We report the levetiracetam pharmacokinetic profile of a patient being treated with levetiracetam 1000 mg intravenously every 12 h who required continuous veno-venous hemofiltration (CVVH). The patient underwent CVVH utilizing a high-flux polyethersulfone membrane filter. The blood flow rate was 250 ml/min, and the predilution replacement therapy fluid flow rate was 2000 ml/h. After achieving presumed steady-state on levetiracetam 1000 mg q12h, serial plasma samples (pre- and post-filter) and effluent samples were drawn at 2, 4, 6, 8, and 10 h. Levetiracetam concentrations were determined utilizing LC-MS/MS. The levetiracetam maximum concentration (Cmax), minimum concentration (Cmin), half-life, area under the concentration-time curve (AUC0-12), clearance (CL), and volume of distribution (Vd) were 30.7 µg/ml, 16.1 µg/ml, 12.9 h, 272 mg·hr/L, 3.68 L/h, and 0.73 L/kg, respectively. The sieving coefficient was 1.03±0.08. CVVH represented 61.3% of the total levetiracetam clearance. The patient was maintained on CVVH for 24 consecutive days and then transitioned to intermittent hemodialysis and remained seizure-free. CONCLUSIONS CVVH is highly effective in removing levetiracetam from circulating plasma. Due to the effective removal, standard doses of levetiracetam are required to maintain adequate plasma concentrations. Dose reductions utilizing HD or estimated creatinine clearance recommendations will likely lead to subtherapeutic levels, especially if higher CVVH flow rates are used.
背景 左乙拉西坦是一种常用于重症患者的抗癫痫药物。左乙拉西坦主要作为母体化合物通过肾小球滤过消除,在肾功能不全时需要调整剂量,但关于接受持续静静脉血液滤过(CVVH)患者的文献较少。病例报告 我们报告了一名每12小时静脉注射1000mg左乙拉西坦且需要持续静静脉血液滤过(CVVH)的患者的左乙拉西坦药代动力学特征。该患者使用高通量聚醚砜膜滤器进行CVVH。血流速度为250ml/分钟,预稀释置换治疗液流速为2000ml/小时。在1000mg q12h的左乙拉西坦达到假定稳态后,在2、4、6、8和10小时采集系列血浆样本(滤器前和滤器后)和流出液样本。使用LC-MS/MS测定左乙拉西坦浓度。左乙拉西坦的最大浓度(Cmax)、最小浓度(Cmin)、半衰期、浓度-时间曲线下面积(AUC0-12)、清除率(CL)和分布容积(Vd)分别为30.7μg/ml、16.1μg/ml、12.9小时、272mg·hr/L、3.68L/小时和0.73L/kg。筛系数为1.03±0.08。CVVH占左乙拉西坦总清除率的61.3%。该患者连续24天维持CVVH治疗,然后转为间歇性血液透析,且未再发生癫痫发作。结论 CVVH在从循环血浆中清除左乙拉西坦方面非常有效。由于清除有效,需要标准剂量的左乙拉西坦来维持足够的血浆浓度。利用血液透析或估计的肌酐清除率建议减少剂量可能会导致治疗水平不足,特别是如果使用更高的CVVH流速。