Traynelis Vincent C, Malone Hani R, Smith Zachary A, Hsu Wellington K, Kanter Adam S, Qureshi Sheeraz A, Cho Samuel K, Baird Evan O, Isaacs Robert E, Rahman Ra'Kerry K, Polevaya Galina, Smith Justin S, Shaffrey Christopher, Tortolani P Justin, Stroh D Alex, Arnold Paul M, Fehlings Michael G, Mroz Thomas E, Riew K Daniel
Rush University Medical Center, Chicago, IL, USA.
Northwestern University, Chicago, IL, USA.
Global Spine J. 2017 Apr;7(1 Suppl):103S-108S. doi: 10.1177/2192568216688184. Epub 2017 Apr 1.
A multicenter retrospective case series.
Horner's syndrome is a known complication of anterior cervical spinal surgery, but it is rarely encountered in clinical practice. To better understand the incidence, risks, and neurologic outcomes associated with Horner's syndrome, a multicenter study was performed to review a large collective experience with this rare complication.
We conducted a retrospective multicenter case series study involving 21 high-volume surgical centers from the AOSpine North America Clinical Research Network. Medical records for 17 625 patients who received subaxial cervical spine surgery from 2005 to 2011 were reviewed to identify occurrence of 21 predefined treatment complications. Descriptive statistics were provided for baseline patient characteristics. Paired test was used to analyze changes in clinical outcomes at follow-up compared to preoperative status.
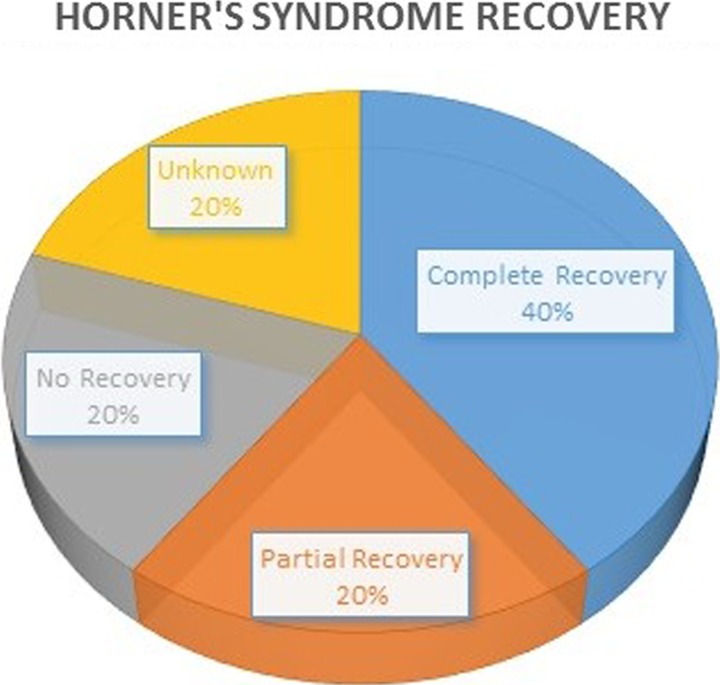
In total, 8887 patients who underwent anterior cervical spine surgery at the participating institutions were screened. Postoperative Horner's syndrome was identified in 5 (0.06%) patients. All patients experienced the complication following anterior cervical discectomy and fusion. The sympathetic trunk appeared to be more vulnerable when operating on midcervical levels (C5, C6), and most patients experienced at least a partial recovery without further treatment.
This collective experience suggests that Horner's syndrome is an exceedingly rare complication following anterior cervical spine surgery. Injury to the sympathetic trunk may be limited by maintaining a midline surgical trajectory when possible, and performing careful dissection and retraction of the longus colli muscle when lateral exposure is necessary, especially at caudal cervical levels.
多中心回顾性病例系列研究。
霍纳综合征是颈椎前路手术已知的一种并发症,但在临床实践中很少见。为了更好地了解与霍纳综合征相关的发病率、风险和神经学结果,开展了一项多中心研究,以回顾关于这种罕见并发症的大量综合经验。
我们进行了一项回顾性多中心病例系列研究,涉及北美脊柱外科学会临床研究网络的21个高手术量的外科中心。回顾了2005年至2011年接受下颈椎手术的17625例患者的病历,以确定21种预先定义的治疗并发症的发生情况。提供了患者基线特征的描述性统计数据。使用配对检验分析随访时与术前状态相比临床结果的变化。
总共筛查了在参与机构接受颈椎前路手术的8887例患者。5例(0.06%)患者被诊断为术后霍纳综合征。所有患者均在颈椎前路椎间盘切除融合术后出现该并发症。在颈椎中段(C5、C6)手术时,交感干似乎更容易受到损伤,大多数患者未经进一步治疗至少有部分恢复。
这一综合经验表明,霍纳综合征是颈椎前路手术后极为罕见的并发症。通过尽可能保持中线手术路径,并在需要侧方暴露时,特别是在颈椎下段,仔细分离和牵开颈长肌,可限制对交感干的损伤。