Huddart Robert A, Birtle Alison, Maynard Lauren, Beresford Mark, Blazeby Jane, Donovan Jenny, Kelly John D, Kirkbank Tony, McLaren Duncan B, Mead Graham, Moynihan Clare, Persad Raj, Scrase Christopher, Lewis Rebecca, Hall Emma
The Institute of Cancer Research, London, UK.
Royal Marsden NHS Foundation Trust, London, UK.
BJU Int. 2017 Nov;120(5):639-650. doi: 10.1111/bju.13900. Epub 2017 May 29.
To test the feasibility of a randomised trial in muscle-invasive bladder cancer (MIBC) and compare outcomes in patients who receive neoadjuvant chemotherapy followed by radical cystectomy (RC) or selective bladder preservation (SBP), where definitive treatment [RC or radiotherapy (RT)] is determined by response to chemotherapy.
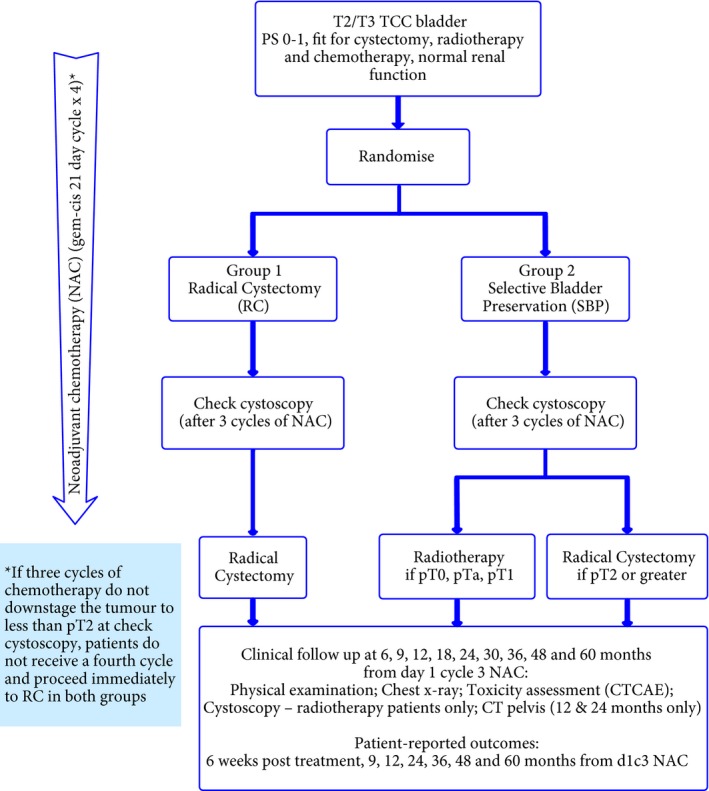
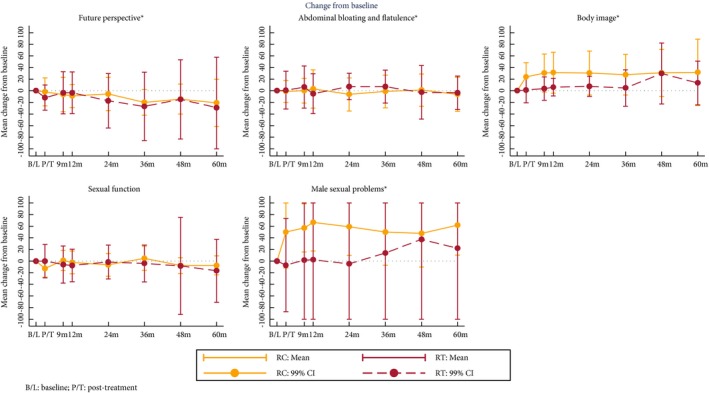
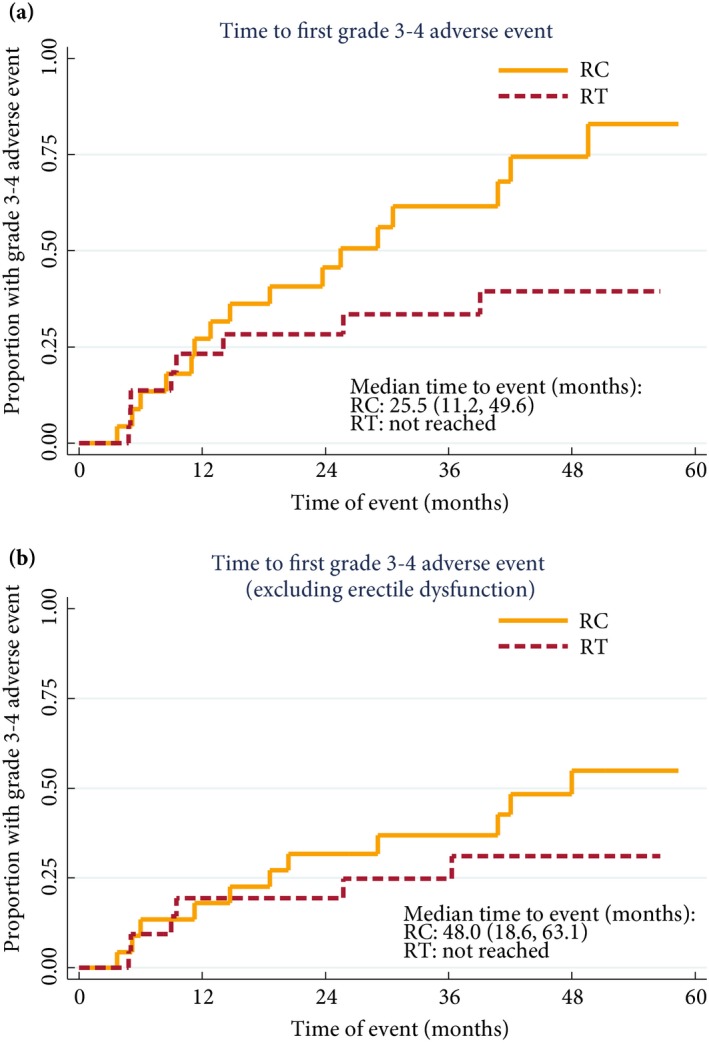
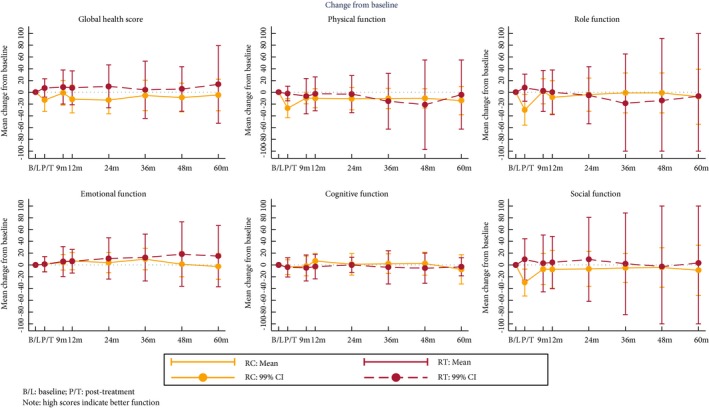
SPARE is a multicentre randomised controlled trial comparing RC and SBP in patients with MIBC staged T2-3 N0 M0, fit for both treatment strategies and receiving three cycles of neoadjuvant chemotherapy. Patients were randomised between RC and SBP before a cystoscopy after cycle three of neoadjuvant chemotherapy. Patients with ≤T1 residual tumour received a fourth cycle of neoadjuvant chemotherapy in both groups, followed by radical RT in the SBP group and RC in in the RC group; non-responders in both groups proceeded immediately to RC following cycle three. Feasibility study primary endpoints were accrual rate and compliance with assigned treatment strategy. The phase III trial was designed to demonstrate non-inferiority of SBP in terms of overall survival (OS) in patients whose tumours responded to neoadjuvant chemotherapy. Secondary endpoints included patient-reported quality of life, clinician assessed toxicity, loco-regional recurrence-free survival, and rate of salvage RC after SBP.
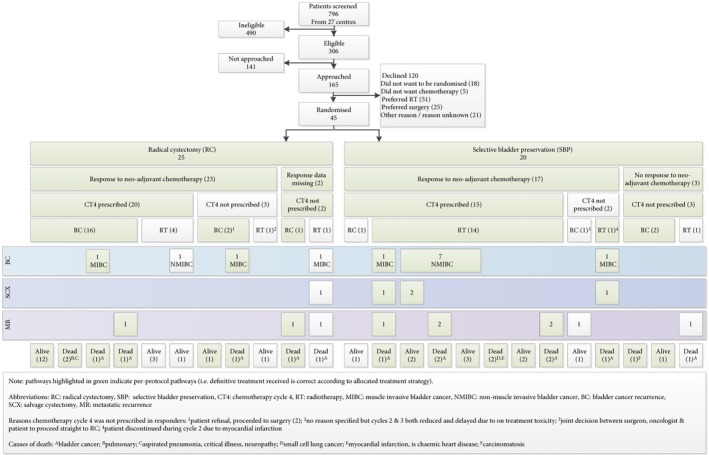
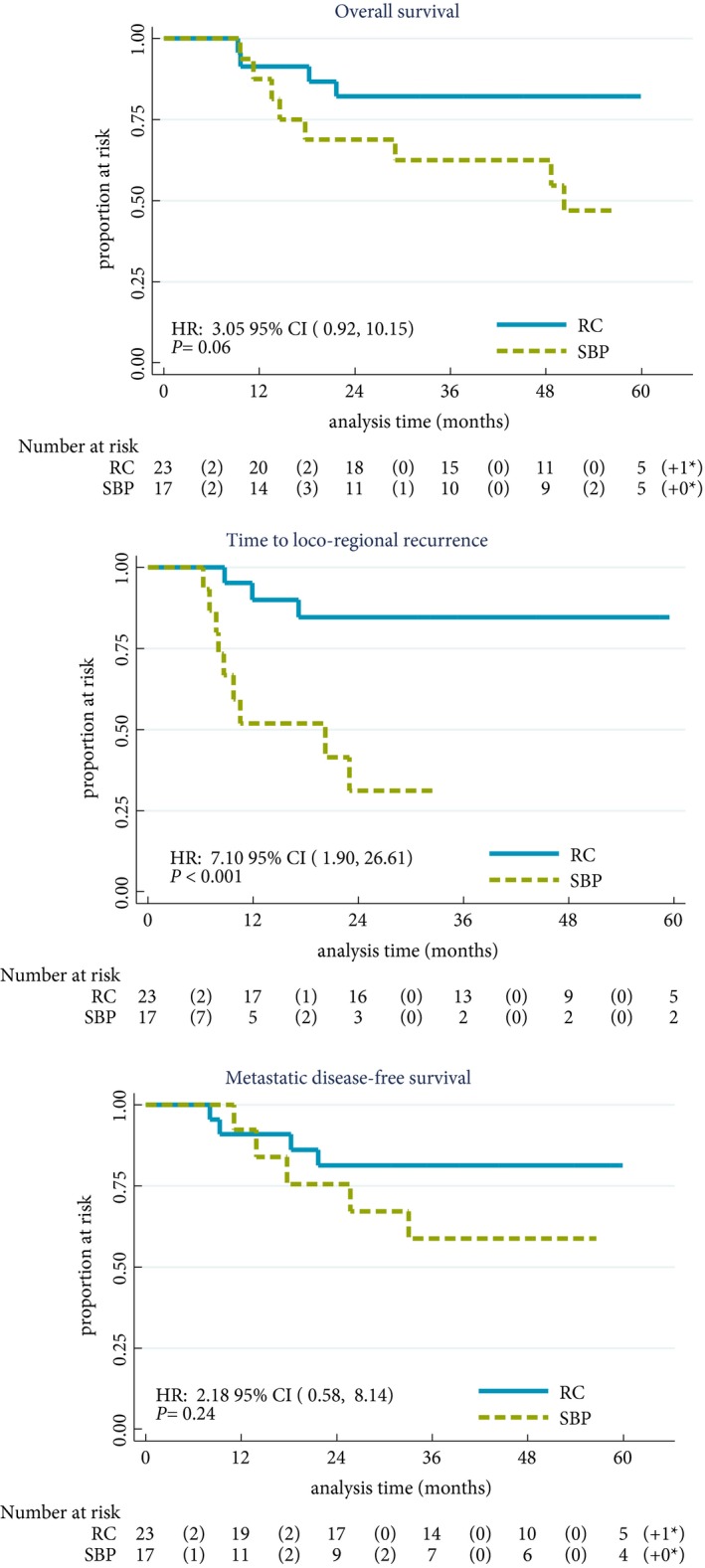
Trial recruitment was challenging and below the predefined target with 45 patients recruited in 30 months (25 RC; 20 SBP). Non-compliance with assigned treatment strategy was frequent, six of the 25 patients (24%) randomised to RC received RT. Long-term bladder preservation rate was 11/15 (73%) in those who received RT per protocol. OS survival was not significantly different between groups.
Randomising patients with MIBC between RC and SBP based on response to neoadjuvant chemotherapy was not feasible in the UK health system. Strong clinician and patient preferences for treatments impacted willingness to undergo randomisation and acceptance of treatment allocation. Due to the few participants, firm conclusions about disease and toxicity outcomes cannot be drawn.
检验在肌肉浸润性膀胱癌(MIBC)中进行一项随机试验的可行性,并比较接受新辅助化疗后行根治性膀胱切除术(RC)或选择性膀胱保留术(SBP)患者的结局,其中确定性治疗[RC或放疗(RT)]由化疗反应决定。
SPARE是一项多中心随机对照试验,比较T2-3 N0 M0期MIBC患者中RC和SBP的疗效,这些患者适合两种治疗策略且接受三个周期的新辅助化疗。在新辅助化疗的第三个周期后进行膀胱镜检查之前,患者被随机分配至RC组和SBP组。两组中残余肿瘤≤T1的患者均接受第四个周期的新辅助化疗,随后SBP组行根治性放疗,RC组行RC;两组中化疗无反应者在第三个周期后立即进行RC。可行性研究的主要终点是入组率和对指定治疗策略的依从性。III期试验旨在证明在肿瘤对新辅助化疗有反应的患者中,SBP在总生存期(OS)方面不劣于RC。次要终点包括患者报告的生活质量、临床医生评估的毒性、局部区域无复发生存期以及SBP后挽救性RC的发生率。
试验招募具有挑战性,未达到预定目标,在30个月内招募了45例患者(25例行RC;20例行SBP)。对指定治疗策略的不依从很常见,随机分配至RC组中的25例患者中有6例(24%)接受了放疗。按照方案接受放疗的患者长期膀胱保留率为11/15(73%)。两组之间的OS无显著差异。
在英国医疗系统中,基于对新辅助化疗的反应在MIBC患者中进行RC和SBP的随机分组是不可行的。临床医生和患者对治疗的强烈偏好影响了接受随机分组和接受治疗分配的意愿。由于参与者较少,无法就疾病和毒性结局得出确凿结论。