Jack Clifford R, Wiste Heather J, Weigand Stephen D, Therneau Terry M, Knopman David S, Lowe Val, Vemuri Prashanthi, Mielke Michelle M, Roberts Rosebud O, Machulda Mary M, Senjem Matthew L, Gunter Jeffrey L, Rocca Walter A, Petersen Ronald C
Department of Radiology, Mayo Clinic, Rochester, MN, USA.
Department of Health Sciences Research, Mayo Clinic, Rochester, MN, USA.
Lancet Neurol. 2017 Jun;16(6):435-444. doi: 10.1016/S1474-4422(17)30077-7. Epub 2017 Apr 26.
A new classification for biomarkers in Alzheimer's disease and cognitive ageing research is based on grouping the markers into three categories: amyloid deposition (A), tauopathy (T), and neurodegeneration or neuronal injury (N). Dichotomising these biomarkers as normal or abnormal results in eight possible profiles. We determined the clinical characteristics and prevalence of each ATN profile in cognitively unimpaired individuals aged 50 years and older.
All participants were in the Mayo Clinic Study of Aging, a population-based study that uses a medical records linkage system to enumerate all individuals aged 50-89 years in Olmsted County, MN, USA. Potential participants are randomly selected, stratified by age and sex, and invited to participate in cognitive assessments; individuals without medical contraindications are invited to participate in brain imaging studies. Participants who were judged clinically as having no cognitive impairment and underwent multimodality imaging between Oct 11, 2006, and Oct 5, 2016, were included in the current study. Participants were classified as having normal (A-) or abnormal (A+) amyloid using amyloid PET, normal (T-) or abnormal (T+) tau using tau PET, and normal (N-) or abnormal (N+) neurodegeneration or neuronal injury using cortical thickness assessed by MRI. We used the cutoff points of standard uptake value ratio (SUVR) 1·42 (centiloid 19) for amyloid PET, 1·23 SUVR for tau PET, and 2·67 mm for MRI cortical thickness. Age-specific and sex-specific prevalences of the eight groups were determined using multinomial models combining data from 435 individuals with amyloid PET, tau PET, and MRI assessments, and 1113 individuals who underwent amyloid PET and MRI, but not tau PET imaging.
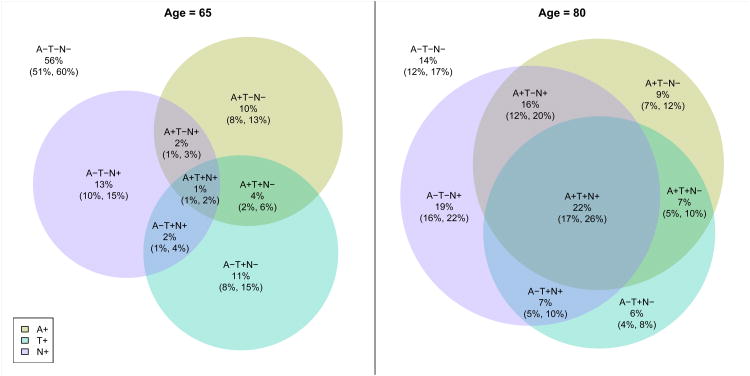
The numbers of participants in each profile group were 165 A-T-N-, 35 A-T+N-, 63 A-T-N+, 19 A-T+N+, 44 A+T-N-, 25 A+T+N-, 35 A+T-N+, and 49 A+T+N+. Age differed by ATN group (p<0·0001), ranging from a median 58 years (IQR 55-64) in A-T-N- and 57 years (54-64) in A-T+N- to a median 80 years (75-84) in A+T-N+ and 79 years (73-87) in A+T+N+. The number of APOE ε4 carriers differed by ATN group (p=0·04), with carriers roughly twice as frequent in each A+ group versus the corresponding A- group. White matter hyperintensity volume (p<0·0001) and cognitive performance (p<0·0001) also differed by ATN group. Tau PET and neurodegeneration biomarkers were discordant in most individuals who would be categorised as stage 2 or 3 preclinical Alzheimer's disease (A+T+N-, A+T-N+, and A+T+N+; 86% at age 65 years and 51% at age 80 years) or with suspected non-Alzheimer's pathophysiology (A-T+N-, A-T-N+, and A-T+N+; 92% at age 65 years and 78% at age 80 years). From age 50 years, A-T-N- prevalence declined and A+T+N+ and A-T+N+ prevalence increased. In both men and women, A-T-N- was the most prevalent until age late 70s. After about age 80 years, A+T+N+ was most prevalent. By age 85 years, more than 90% of men and women had one or more biomarker abnormalities.
Biomarkers of fibrillar tau deposition can be included with those of β-amyloidosis and neurodegeneration or neuronal injury to more fully characterise the heterogeneous pathological profiles in the population. Both amyloid- dependent and amyloid-independent pathological profiles can be identified in the cognitively unimpaired population. The prevalence of each ATN group changed substantially with age, with progression towards more biomarker abnormalities among individuals who remained cognitively unimpaired.
National Institute on Aging (part of the US National Institutes of Health), the Alexander Family Professorship of Alzheimer's Disease Research, the Mayo Clinic, and the GHR Foundation.
阿尔茨海默病和认知衰老研究中生物标志物的一种新分类方法是将标志物分为三类:淀粉样蛋白沉积(A)、tau蛋白病变(T)和神经退行性变或神经元损伤(N)。将这些生物标志物分为正常或异常会产生八种可能的组合。我们确定了50岁及以上认知未受损个体中每种ATN组合的临床特征和患病率。
所有参与者均来自梅奥诊所衰老研究,这是一项基于人群的研究,使用医疗记录链接系统对美国明尼苏达州奥尔姆斯特德县所有50 - 89岁的个体进行统计。潜在参与者通过年龄和性别分层随机选取,并被邀请参加认知评估;无医学禁忌的个体被邀请参加脑成像研究。在2006年10月11日至2016年10月5日期间,临床判断无认知障碍且接受多模态成像的参与者被纳入本研究。使用淀粉样蛋白PET将参与者分类为淀粉样蛋白正常(A -)或异常(A +),使用tau蛋白PET分类为tau蛋白正常(T -)或异常(T +),使用MRI评估的皮质厚度将神经退行性变或神经元损伤分类为正常(N -)或异常(N +)。我们使用淀粉样蛋白PET的标准摄取值比率(SUVR)1.42(19百分位)、tau蛋白PET的1.23 SUVR以及MRI皮质厚度的2.67 mm作为截断点。使用多项模型结合435名进行淀粉样蛋白PET、tau蛋白PET和MRI评估的个体以及1113名进行淀粉样蛋白PET和MRI但未进行tau蛋白PET成像的个体的数据,确定八组的年龄特异性和性别特异性患病率。
各组合组的参与者人数分别为165例A - T - N -、35例A - T + N -、63例A - T - N +、19例A - T + N +、44例A + T - N -、25例A + T + N -、35例A + T - N +和49例A + T + N +。年龄因ATN组而异(p < 0.0001),范围从A - T - N -组的中位数58岁(IQR 55 - 64)和A - T + N -组的57岁(54 - 64)到A + T - N +组的中位数80岁(75 - 84)和A + T + N +组的79岁(73 - 87)。APOE ε4携带者的数量因ATN组而异(p = 0.04),每个A +组的携带者频率约为相应A -组的两倍。白质高信号体积(p < 0.0001)和认知表现(p < 0.0001)也因ATN组而异。在大多数将被归类为临床前阿尔茨海默病2期或3期(A + T + N -)、A + T - N +和A + T + N +;65岁时为86%,80岁时为51%)或疑似非阿尔茨海默病病理生理(A - T + N -、A - T - N +和A - T + N +;65岁时为92%,80岁时为78%)的个体中,tau蛋白PET和神经退行性变生物标志物不一致。从50岁起,A - T - N -患病率下降,A + T + N +和A - T + N +患病率增加。在男性和女性中,A - T - N -在7旬后期之前最为常见。大约80岁以后,A + T + N +最为常见。到85岁时,超过90%的男性和女性有一个或多个生物标志物异常。
纤维状tau蛋白沉积的生物标志物可与β -淀粉样变性以及神经退行性变或神经元损伤的生物标志物一起,更全面地描述人群中异质性病理特征。在认知未受损人群中可识别出依赖淀粉样蛋白和不依赖淀粉样蛋白的病理特征。每个ATN组的患病率随年龄大幅变化,在认知未受损个体中朝着更多生物标志物异常发展。
美国国立衰老研究所(美国国立卫生研究院的一部分)、亚历山大家族阿尔茨海默病研究教授职位、梅奥诊所和GHR基金会。