Department of Radiology, Mayo Clinic, Rochester, MN, USA.
Department of Health Sciences Research, Mayo Clinic, Rochester, MN, USA.
Brain. 2019 Oct 1;142(10):3230-3242. doi: 10.1093/brain/awz268.
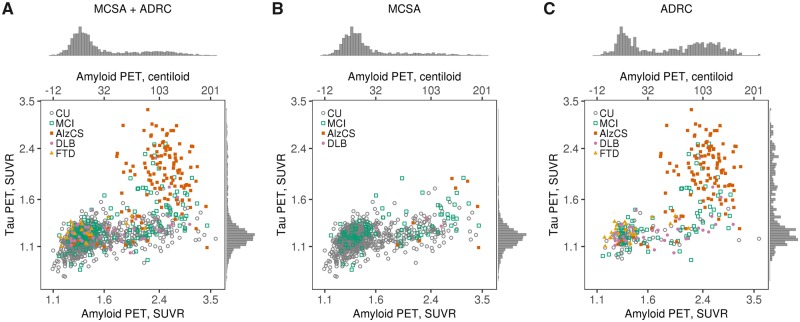
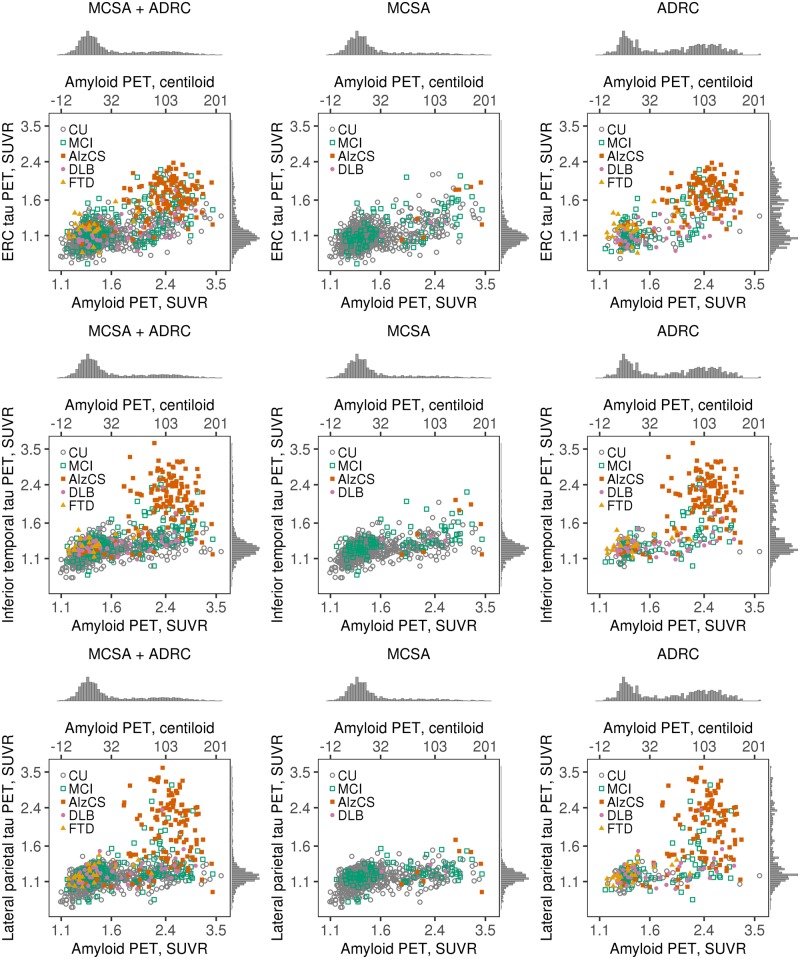
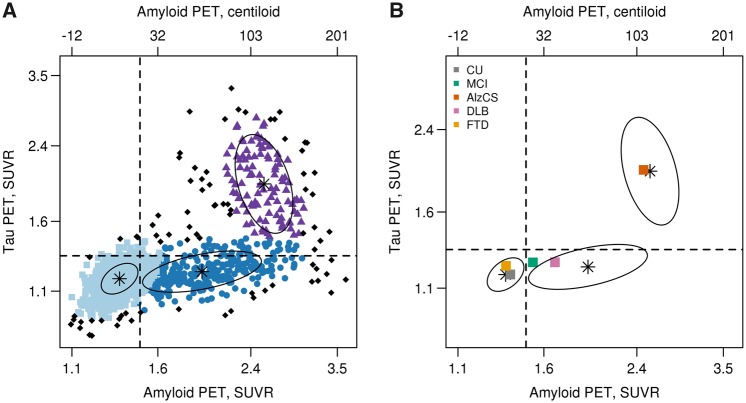
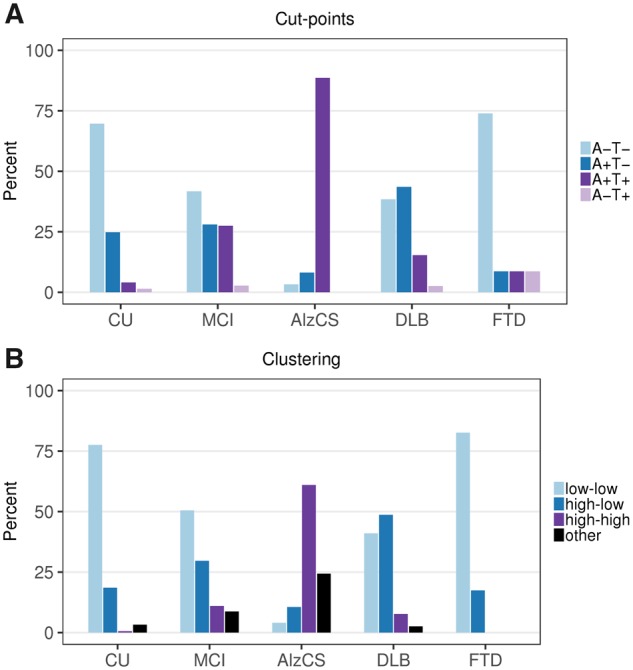
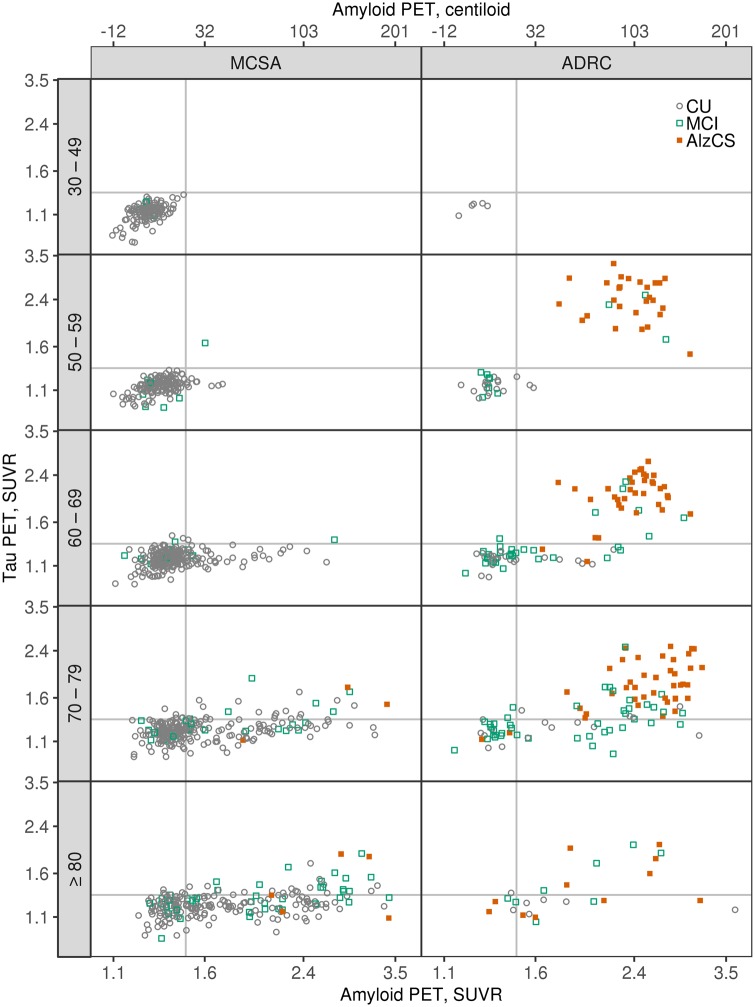
Large phenotypically diverse research cohorts with both amyloid and tau PET have only recently come into existence. Our objective was to determine relationships between the bivariate distribution of amyloid-β and tau on PET and established clinical syndromes that are relevant to cognitive ageing and dementia. All individuals in this study were enrolled in the Mayo Clinic Study of Aging, a longitudinal population-based study of cognitive ageing, or the Mayo Alzheimer Disease Research Center, a longitudinal study of individuals recruited from clinical practice. We studied 1343 participants who had amyloid PET and tau PET from 2 April 2015 to 3 May 2019, and met criteria for membership in one of five clinical diagnostic groups: cognitively unimpaired, mild cognitive impairment, frontotemporal dementia, probable dementia with Lewy bodies, and Alzheimer clinical syndrome. We examined these clinical groups in relation to the bivariate distribution of amyloid and tau PET values. Individuals were grouped into amyloid (A)/tau (T) quadrants based on previously established abnormality cut points of standardized uptake value ratio 1.48 (A) and 1.33 (T). Individual participants largely fell into one of three amyloid/tau quadrants: low amyloid and low tau (A-T-), high amyloid and low tau (A+T-), or high amyloid and high tau (A+T+). Seventy per cent of cognitively unimpaired and 74% of FTD participants fell into the A-T- quadrant. Participants with mild cognitive impairment spanned the A-T- (42%), A+T- (28%), and A+T+ (27%) quadrants. Probable dementia with Lewy body participants spanned the A-T- (38%) and A+T- (44%) quadrants. Most (89%) participants with Alzheimer clinical syndrome fell into the A+T+ quadrant. These data support several conclusions. First, among 1343 participants, abnormal tau PET rarely occurred in the absence of abnormal amyloid PET, but the reverse was common. Thus, with rare exceptions, amyloidosis appears to be required for high levels of 3R/4R tau deposition. Second, abnormal amyloid PET is compatible with normal cognition but highly abnormal tau PET is not. These two conclusions support a dynamic biomarker model in which Alzheimer's disease is characterized first by the appearance of amyloidosis and later by tauopathy, with tauopathy being the proteinopathy associated with clinical symptoms. Third, bivariate amyloid and tau PET relationships differed across clinical groups and thus have a role for clarifying the aetiologies underlying neurocognitive clinical syndromes.
大型表型多样的研究队列,同时具有淀粉样蛋白和 tau PET 数据,直到最近才出现。我们的目标是确定 PET 上淀粉样蛋白-β和 tau 的双变量分布与认知老化和痴呆相关的既定临床综合征之间的关系。本研究中的所有个体均纳入 Mayo 诊所老龄化研究,这是一项针对认知老化的纵向基于人群的研究,或 Mayo 阿尔茨海默病研究中心,这是一项从临床实践中招募个体的纵向研究。我们研究了 1343 名参与者,他们在 2015 年 4 月 2 日至 2019 年 5 月 3 日期间进行了淀粉样蛋白 PET 和 tau PET,并且符合以下五个临床诊断组之一的成员标准:认知正常、轻度认知障碍、额颞叶痴呆、可能的路易体痴呆症和阿尔茨海默病临床综合征。我们检查了这些临床组与淀粉样蛋白和 tau PET 值的双变量分布的关系。根据先前建立的标准化摄取比值 1.48(A)和 1.33(T)的异常截断点,将个体分为淀粉样蛋白(A)/tau(T)象限。个体参与者主要分为以下三个淀粉样蛋白/ tau 象限之一:低淀粉样蛋白和低 tau(A-T-)、高淀粉样蛋白和低 tau(A+T-)或高淀粉样蛋白和高 tau(A+T+)。70%的认知正常和 74%的额颞叶痴呆参与者属于 A-T-象限。轻度认知障碍患者跨越 A-T-(42%)、A+T-(28%)和 A+T+(27%)象限。可能的路易体痴呆症参与者跨越 A-T-(38%)和 A+T-(44%)象限。大多数(89%)阿尔茨海默病临床综合征患者属于 A+T+象限。这些数据支持几个结论。首先,在 1343 名参与者中,异常 tau PET 很少在没有异常淀粉样蛋白 PET 的情况下发生,但反之则很常见。因此,除了极少数例外,淀粉样蛋白病似乎是 3R/4R tau 沉积高水平所必需的。其次,异常淀粉样蛋白 PET 与认知正常相容,但高度异常的 tau PET 则不然。这两个结论支持一个动态生物标志物模型,即阿尔茨海默病首先表现为淀粉样蛋白病,随后表现为 tau 病,tau 病是与临床症状相关的蛋白病。第三,淀粉样蛋白和 tau PET 的双变量关系因临床组而异,因此在阐明神经认知临床综合征的病因方面具有作用。