McBrien Kerry A, Naugler Christopher, Ivers Noah, Weaver Robert G, Campbell David, Desveaux Laura, Hemmelgarn Brenda R, Edwards Alun L, Saad Nathalie, Nicholas David, Manns Braden J
Department of Family Medicine, Cumming School of Medicine, University of Calgary, Calgary, Canada.
Department of Community Health Sciences, Cumming School of Medicine, University of Calgary, Calgary, Canada.
PLoS One. 2017 May 1;12(5):e0176135. doi: 10.1371/journal.pone.0176135. eCollection 2017.
To determine and quantify the prevalence of patient, provider and system level barriers to achieving diabetes care goals; and to examine whether barriers were different for people with poor glycemic control (HbA1c ≥ 10%; 86 mmol/mol) compared to fair glycemic control (7 to <8%; 53-64 mmol/mol).
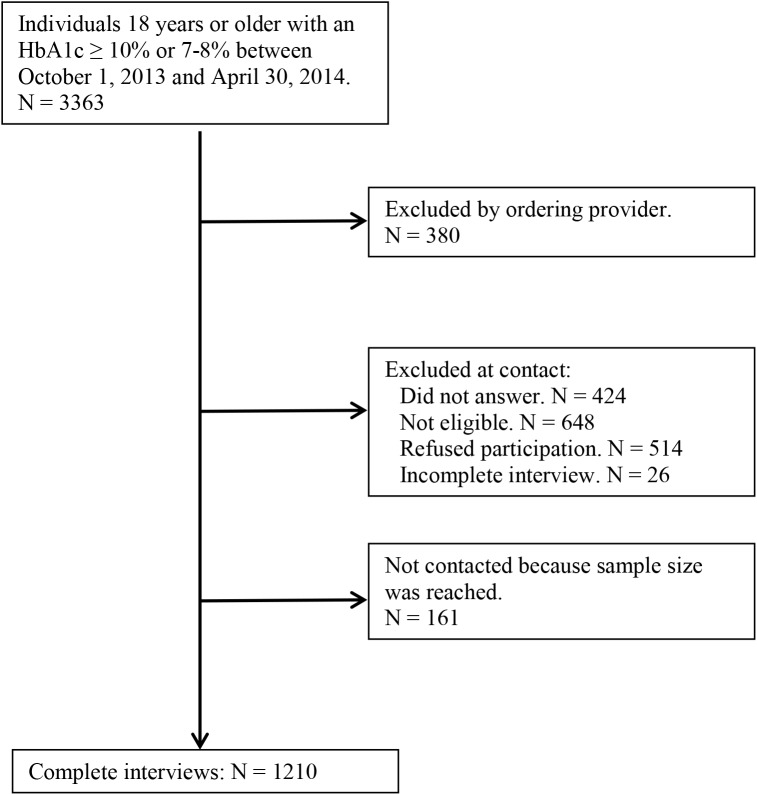
We administered a survey by telephone to community-dwelling patients with diabetes, to examine patient-reported barriers and facilitators to care. We compared responses in individuals with HbA1c ≥ 10% (86 mmol/mol) against those with HbA1c between 7-8% (53-64 mmol/mol). We examined associations between HbA1c group and barriers to care, adjusting for sociodemographic factors and diabetes duration.
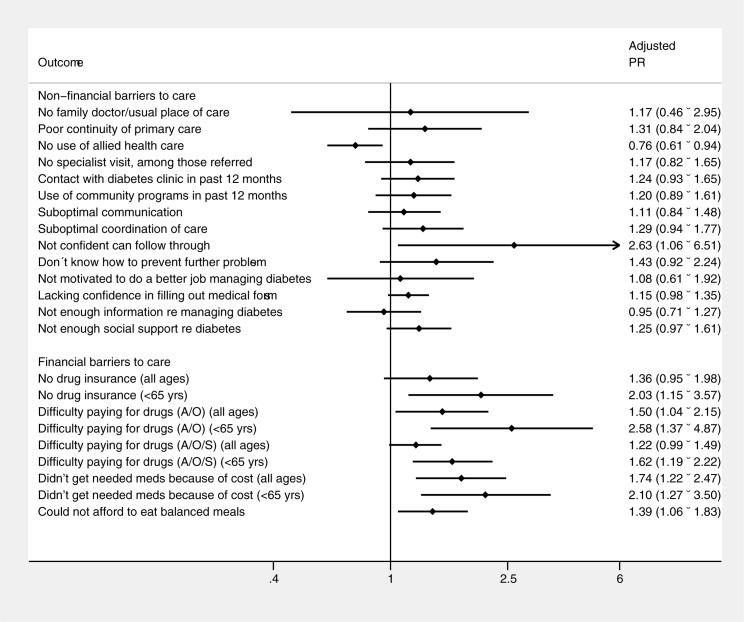
The survey included 805 people with HbA1c ≥ 10% (86 mmol/mol), and 405 people with HbA1c 7-8% (53-64 mmol/mol). Participants with HbA1c ≥ 10% (86 mmol/mol) reported good access to care, however 20% of participants with HbA1c ≥ 10% (86 mmol/mol) felt that their care was not well-coordinated and 9.6% reported having an unmet health care need. In adjusted analysis, patients with HbA1c ≥10% (86 mmol/mol) were more likely to report lack of confidence and inadequate social support, compared to patients with HbA1c 7-8% (53-64 mmol/mol). They were also significantly more likely not to have drug insurance nor to have received recommended treatments because of cost.
These results reinforce the importance of an individualized, yet multi-faceted approach. Specific attention to financial barriers seems warranted. These findings can inform the development of programs and initiatives to overcome barriers to care, and improve diabetes care and outcomes.
确定并量化实现糖尿病护理目标过程中患者、医护人员和系统层面的障碍发生率;并研究血糖控制不佳(糖化血红蛋白≥10%;86 mmol/mol)的人群与血糖控制尚可(7%至<8%;53 - 64 mmol/mol)的人群相比,障碍是否存在差异。
我们通过电话对社区居住的糖尿病患者进行了一项调查,以检查患者报告的护理障碍和促进因素。我们将糖化血红蛋白≥10%(86 mmol/mol)的个体与糖化血红蛋白在7% - 8%(53 - 64 mmol/mol)之间的个体的回答进行了比较。我们研究了糖化血红蛋白分组与护理障碍之间的关联,并对社会人口学因素和糖尿病病程进行了调整。
该调查纳入了805名糖化血红蛋白≥10%(86 mmol/mol)的患者和405名糖化血红蛋白7% - 8%(53 - 64 mmol/mol)的患者。糖化血红蛋白≥10%(86 mmol/mol)的参与者表示获得护理的机会良好,然而,20%糖化血红蛋白≥10%(86 mmol/mol)的参与者认为他们的护理协调不佳,9.6%的参与者报告有未满足的医疗需求。在调整分析中,与糖化血红蛋白7% - 8%(53 - 64 mmol/mol)的患者相比,糖化血红蛋白≥10%(86 mmol/mol)的患者更有可能报告缺乏信心和社会支持不足。他们也显著更有可能没有药物保险,或因费用问题未接受推荐的治疗。
这些结果强化了个体化且多方面方法的重要性。似乎有必要特别关注经济障碍。这些发现可为制定克服护理障碍、改善糖尿病护理及结局的项目和举措提供参考。