Liu Peter, Dillingham Rebecca, McManus Kathleen
Department of Internal Medicine, University of Virginia, PO Box 801379, Charlottesville, VA 22908 USA.
Division of Infectious Diseases and International Health, University of Virginia, PO Box 801379, Charlottesville, VA 22908 USA.
AIDS Res Ther. 2017 May 2;14:25. doi: 10.1186/s12981-017-0152-0. eCollection 2017.
Immune reconstitution inflammatory syndrome (IRIS) can manifest with initiation or reintroduction of antiretroviral therapy (ART) in persons living with HIV (PLWH). In 2012, updated United States treatment guidelines recommended initiation of ART for all PLWH regardless of CD4 count. The objectives of this study were to quantify hospital usage attributable to IRIS and assess the reasons for hospitalization in PLWH before and after the guideline update.
Subjects were PLWH between 18-89 years of age who were hospitalized between November 1, 2009 and July 31, 2014. Equivalent time periods before and after updated treatment guidelines were considered, and designated as Time Period 1 and Time Period 2, respectively. IRIS-attributable hospitalizations were identified by ICD9 codes and electronic medical record searches with subsequent review and confirmation. For hospitalizations that were not confirmed as being IRIS-attributable, primary discharge diagnoses were reviewed.
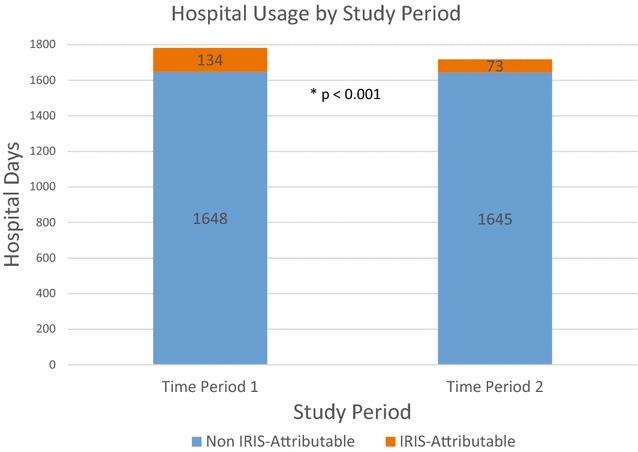
A total of 278 PLWH were hospitalized 521 times throughout the study period. Time Period 1 had 9 PLWH with 12 IRIS-attributable hospitalizations while Time Period 2 had 6 PLWH with 9 IRIS-attributable hospitalizations. A larger proportion of IRIS-attributable hospital days was observed in Time Period 1 compared to Time Period 2 (7.5 vs 4.2%; p < 0.001). Median length of stay for IRIS-attributable hospitalizations was longer than for other diagnoses, particularly during Time Period 1 (12.0 vs 4.0; p = 0.05). The most common causes for hospitalizations in PLWH were non AIDS-defining infection, AIDS-defining malignancy, and gastrointestinal. PLWH who had HIV viral suppression (<200 copies/mL) accounted for 34 and 24% of hospitalizations in Time Periods 1 and 2 respectively.
Hospitalizations for PLWH continue at high rates and IRIS is a significant contributing factor. In our single-center study, there was a lower number of IRIS-attributable hospitalizations and IRIS-attributable hospital days in Time Period 2 compared with Time Period 1. The hospital burden of IRIS may decrease over time as more PLWH are started on ART earlier in the course of infection. This study highlights the continued importance of early diagnosis and linkage to care of those infected with HIV, so that morbidity and costs associated with IRIS continue to decline.
免疫重建炎症综合征(IRIS)可在接受抗逆转录病毒治疗(ART)的HIV感染者(PLWH)开始治疗或重新接受治疗时出现。2012年,美国更新的治疗指南建议所有PLWH无论CD4细胞计数如何均开始接受ART治疗。本研究的目的是量化IRIS导致的住院情况,并评估指南更新前后PLWH住院的原因。
研究对象为年龄在18 - 89岁之间、于2009年11月1日至2014年7月31日期间住院的PLWH。考虑更新治疗指南前后的等效时间段,分别指定为时间段1和时间段2。通过ICD9编码和电子病历搜索确定IRIS相关的住院病例,随后进行审查和确认。对于未确认为IRIS相关的住院病例,审查主要出院诊断。
在整个研究期间,共有278名PLWH住院521次。时间段1有9名PLWH发生12次IRIS相关住院,而时间段2有6名PLWH发生9次IRIS相关住院。与时间段2相比,时间段1中IRIS相关住院天数的比例更高(7.5%对4.2%;p < 0.001)。IRIS相关住院的中位住院时间长于其他诊断,特别是在时间段1(12.0天对4.0天;p = 0.05)。PLWH住院的最常见原因是非艾滋病定义性感染、艾滋病定义性恶性肿瘤和胃肠道疾病。HIV病毒得到抑制(<200拷贝/mL)的PLWH分别占时间段1和时间段2住院病例的34%和24%。
PLWH的住院率仍然很高,IRIS是一个重要的促成因素。在我们的单中心研究中,与时间段1相比,时间段2中IRIS相关住院病例数和IRIS相关住院天数较少。随着越来越多的PLWH在感染过程中更早开始接受ART治疗,IRIS的住院负担可能会随着时间的推移而降低。本研究强调了对HIV感染者进行早期诊断和与护理机构建立联系的持续重要性,以便与IRIS相关的发病率和成本继续下降。