Beau Anna-Belle, Lynge Elsebeth, Njor Sisse Helle, Vejborg Ilse, Lophaven Søren Nymand
Department of Public Health, University of Copenhagen, DK-1014, Copenhagen, Denmark.
Department of Clinical Epidemiology, University of Aarhus, DK-8200, Aarhus, Denmark.
Int J Cancer. 2017 Aug 1;141(3):512-518. doi: 10.1002/ijc.30758. Epub 2017 May 10.
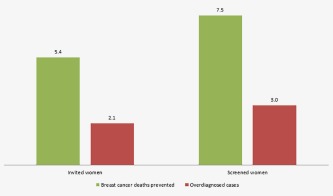
The primary aim of breast cancer screening is to reduce breast cancer mortality, but screening also has negative side-effects as overdiagnosis. To evaluate a screening programme, both benefits and harms should be considered. Published estimates of the benefit-to-harm ratio, the number of breast cancer deaths prevented divided by the number of overdiagnosed breast cancer cases, varied considerably. The objective of the study was to estimate the benefit-to-harm ratio of breast cancer screening in Denmark. The numbers of breast cancer deaths prevented and overdiagnosed cases [invasive and ductal carcinoma in situ (DCIS)] were estimated per 1,000 women aged 50-79, using national published estimates for breast cancer mortality and overdiagnosis, and national incidence and mortality rates. Estimations were made for both invited and screened women. Among 1,000 women invited to screening from age 50 to age 69 and followed until age 79, we estimated that 5.4 breast cancer deaths would be prevented and 2.1 cases overdiagnosed, under the observed scenario in Denmark of a breast cancer mortality reduction of 23.4% and 2.3% of the breast cancer cases being overdiagnosed. The estimated benefit-to-harm ratio was 2.6 for invited women and 2.5 for screened women. Hence, 2-3 women would be prevented from dying from breast cancer for every woman overdiagnosed with invasive breast cancer or DCIS. The difference between the previous published ratios and 2.6 for Denmark is probably more a reflection of the accuracy of the underlying estimates than of the actual screening programmes. Therefore, benefit-to-harm ratios should be used cautiously.
乳腺癌筛查的主要目标是降低乳腺癌死亡率,但筛查也存在如过度诊断等负面副作用。为评估一项筛查计划,应同时考虑其益处和危害。已发表的益处与危害比的估计值,即预防的乳腺癌死亡人数除以过度诊断的乳腺癌病例数,差异很大。本研究的目的是估计丹麦乳腺癌筛查的益处与危害比。利用国家公布的乳腺癌死亡率和过度诊断估计值以及国家发病率和死亡率,估计每1000名年龄在50 - 79岁的女性中预防的乳腺癌死亡人数和过度诊断的病例数(浸润性癌和导管原位癌)。对受邀参加筛查的女性和实际接受筛查的女性都进行了估计。在1000名年龄从50岁至69岁受邀参加筛查并随访至79岁的女性中,按照丹麦观察到的情况,即乳腺癌死亡率降低23.4%且2.3%的乳腺癌病例被过度诊断,我们估计可预防5.4例乳腺癌死亡,过度诊断2.1例。受邀女性的估计益处与危害比为2.6,接受筛查女性的为2.5。因此,每有一名被过度诊断为浸润性乳腺癌或导管原位癌的女性,就有2 - 3名女性可预防死于乳腺癌。丹麦之前公布的比率与2.6之间的差异,可能更多反映的是基础估计值的准确性,而非实际筛查计划。因此,应谨慎使用益处与危害比。