Aljuboori Zaid, Hruska Rob, Yaseen Alae, Arnold Forest, Wojda Barbara, Nauta Haring
Department of Neurological Surgery, University of Louisville SOM, Louisville, Kentucky, USA.
Department of Pathology, University of Louisville SOM, Louisville, Kentucky, USA.
Surg Neurol Int. 2017 Apr 5;8:46. doi: 10.4103/sni.sni_448_16. eCollection 2017.
Central nervous system infection with (Black Mold) is rare. It carries a high mortality rate, that is more than 70%, despite multimodal therapy.
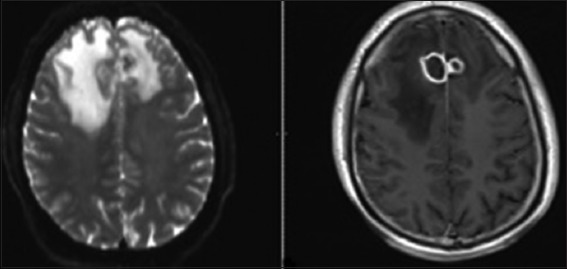
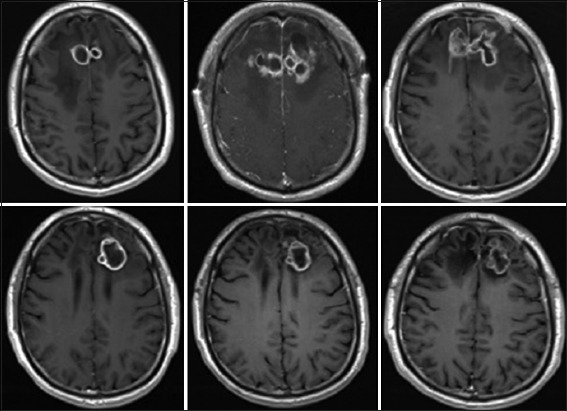
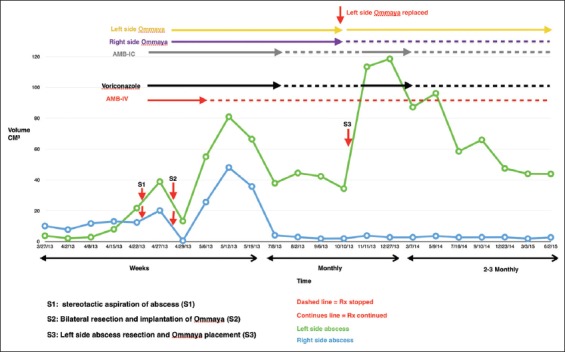
We present a rare case of "black mold" fungal brain abscess that was successfully treated with good patient outcome. The case is unusual because there were two fungal brain abscesses located bilaterally symmetrically in the mesial frontal lobes, and the response to different treatment strategies was well documented by over 25 magnetic resonance imaging (MRI) scans. Initial attempts to treat these lesions by repeated surgical excision and systemic amphotericin B was followed by continued growth rather than resolution. We realized that the application of treatment principles learned from bacterial brain abscess may not transpose intuitively to the treatment of fungal brain abscess. Therefore, a new treatment strategy was adopted that avoided further attempts at resection in favor of long-term oral voriconazole and repeated intracavitary aspiration and instillation of amphotericin B on an outpatient basis. Without further resection, the lesions stabilized and the aspirates eventually sterilized, however, the enhancing capsule never resolved on MRI scans. All treatment was stopped after 1 year. The apparently sterilized lesions have been followed for an additional 3 years without further growth, and the patient remains functionally, intellectually, and behaviorally normal.
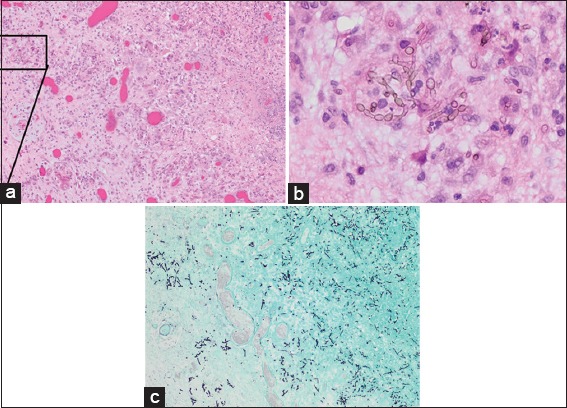
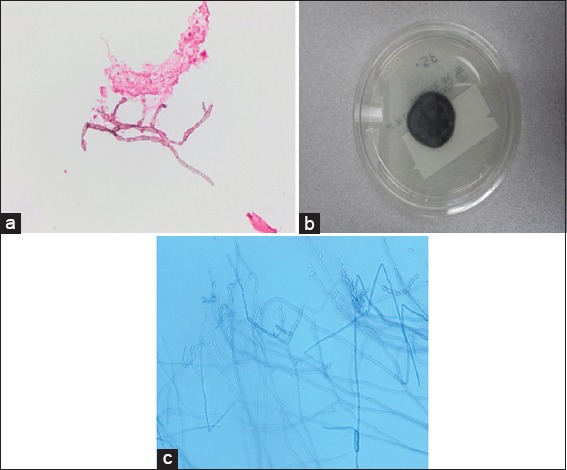
We conclude that, in the case of fungal abscess, it may be preferable to sterilize the lesion rather than attempting to achieve resolution on imaging studies by repeated surgical resection of the capsule which can be counterproductive. This strategy accepts that the capsule may be important to the patient's immune defense against the fungus. Helping that defense barrier with intracapsular and systemic antifungal agents, rather than capsular removal, may be the better strategy for patients in whom early aggressive resection has failed. The basis for the apparent differences in the response of fungal versus bacterial brain abscess to surgical resection is discussed in the light of pathological findings from this and other cases.
中枢神经系统感染(黑霉菌)较为罕见。尽管采用了多模式治疗,但其死亡率仍很高,超过70%。
我们报告一例罕见的“黑霉菌”真菌性脑脓肿,经成功治疗,患者预后良好。该病例不同寻常之处在于,两个真菌性脑脓肿对称地位于双侧额叶内侧,超过25次磁共振成像(MRI)扫描对不同治疗策略的反应进行了充分记录。最初尝试通过反复手术切除和全身使用两性霉素B治疗这些病变,但病变持续生长而非消退。我们意识到,从细菌性脑脓肿中学到的治疗原则可能无法直接应用于真菌性脑脓肿的治疗。因此,我们采用了一种新的治疗策略,即避免进一步切除,转而长期口服伏立康唑,并在门诊反复进行囊内抽吸和两性霉素B注入。无需进一步切除,病变得以稳定,抽吸物最终无菌,但MRI扫描显示强化包膜从未消退。1年后停止所有治疗。对明显无菌的病变又进行了3年的随访,未见进一步生长,患者在功能、智力和行为方面仍保持正常。
我们得出结论,对于真菌性脓肿,使病变无菌化可能比通过反复手术切除包膜在影像学上实现消退更为可取,因为反复手术切除可能适得其反。该策略认为包膜可能对患者抵御真菌的免疫防御很重要。对于早期积极切除失败的患者,通过囊内和全身使用抗真菌药物来增强这种防御屏障,而非切除包膜,可能是更好的策略。结合本病例和其他病例的病理结果,讨论了真菌性与细菌性脑脓肿对手术切除反应明显不同的原因。