Rhee Chanu
Department of Population Medicine, Harvard Medical School/Harvard Pilgrim Health Care Institute, Boston, Massachusetts.
Division of Infectious Diseases, Brigham and Women's Hospital, Boston, Massachusetts.
Open Forum Infect Dis. 2016 Dec 7;4(1):ofw249. doi: 10.1093/ofid/ofw249. eCollection 2017 Winter.
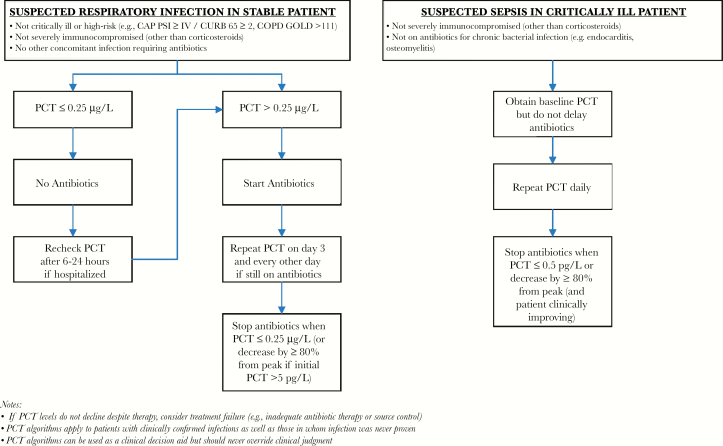
Procalcitonin levels rise in response to systemic inflammation, especially of bacterial origin. Multiple randomized controlled trials have demonstrated that procalcitonin-based algorithms can safely reduce antibiotic use in 2 clinical scenarios. First, in stable, low-risk patients with respiratory infections, procalcitonin levels of <0.25 µg/L can guide the decision to withhold antibiotics or stop therapy early. Second, in critically ill patients with suspected sepsis, clinicians should not initially withhold antibiotics, but procalcitonin levels of <0.5 µg/L or levels that decrease by ≥80% from peak can guide discontinuation once patients stabilize. The recent stop antibiotics on procalcitonin guidance study (SAPS), the largest procalcitonin trial to date, demonstrated reduction in both antibiotic exposure and mortality in critically ill patients. Although procalcitonin is ready for routine use, future research should examine optimal strategies for implementation in hospitals, its real-world impact on clinical outcomes and costs, its applicability to immunocompromised patients, and the generalizability of trials to the US population.
降钙素原水平会因全身炎症反应(尤其是细菌感染引起的)而升高。多项随机对照试验表明,基于降钙素原的算法可在两种临床情况下安全地减少抗生素使用。第一,在患有呼吸道感染的稳定、低风险患者中,降钙素原水平<0.25 µg/L可指导决定停用抗生素或提前终止治疗。第二,在疑似脓毒症的重症患者中,临床医生最初不应停用抗生素,但降钙素原水平<0.5 µg/L或从峰值下降≥80%的水平可在患者病情稳定后指导停药。最近的降钙素原指导下停用抗生素研究(SAPS)是迄今为止规模最大的降钙素原试验,该研究表明重症患者的抗生素暴露和死亡率均有所降低。尽管降钙素原已可用于常规使用,但未来的研究应探讨在医院实施的最佳策略、其对临床结局和成本的实际影响、其对免疫功能低下患者的适用性以及试验结果在美国人群中的可推广性。