Linas Benjamin P, Morgan Jake R, Pho Mai T, Leff Jared A, Schackman Bruce R, Horsburgh C Robert, Assoumou Sabrina A, Salomon Joshua A, Weinstein Milton C, Freedberg Kenneth A, Kim Arthur Y
Section of Infectious Diseases, Department of Medicine, Boston Medical Center, Massachusetts.
Department of Epidemiology, Boston University School of Public Health, Massachusetts.
Open Forum Infect Dis. 2016 Dec 27;4(1):ofw266. doi: 10.1093/ofid/ofw266. eCollection 2017 Winter.
Interferon-free regimens to treat hepatitis C virus (HCV) genotype 1 are effective but costly. At this time, payers in the United States use strategies to control costs including (1) limiting treatment to those with advanced disease and (2) negotiating price discounts in exchange for exclusivity.
We used Monte Carlo simulation to investigate budgetary impact and cost effectiveness of these treatment policies and to identify strategies that balance access with cost control. Outcomes included nondiscounted 5-year payer cost per 10000 HCV-infected patients and incremental cost-effectiveness ratios.
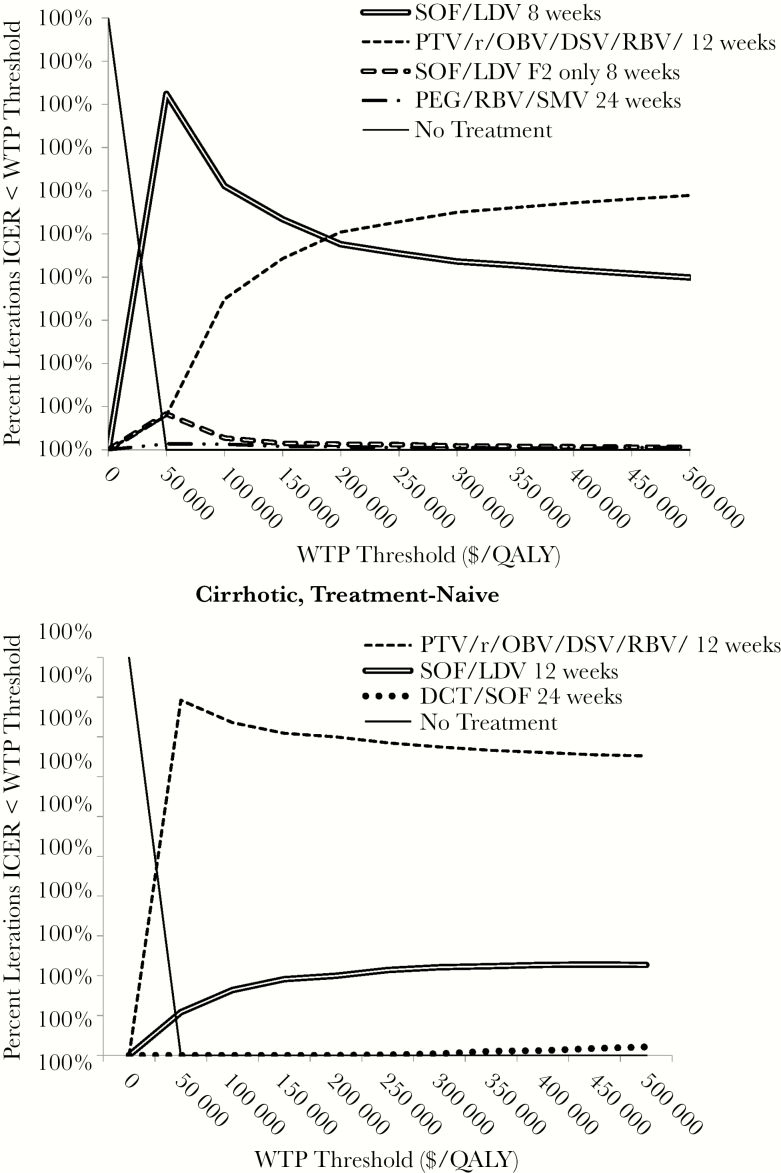
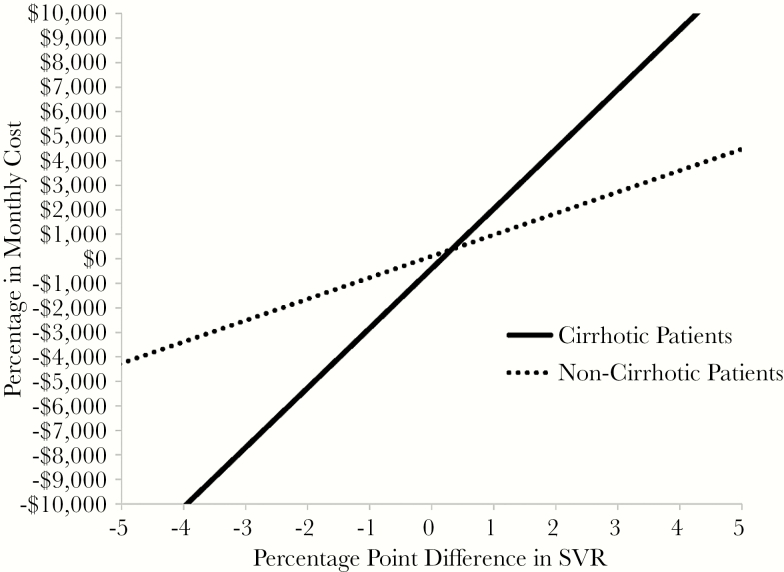
We found that the budgetary impact of HCV treatment is high, with 5-year undiscounted costs of $1.0 billion to 2.3 billion per 10000 HCV-infected patients depending on regimen choices. Among noncirrhotic patients, using the least costly interferon-free regimen leads to the lowest payer costs with negligible difference in clinical outcomes, even when the lower cost regimen is less convenient and/or effective. Among cirrhotic patients, more effective but costly regimens remain cost effective. Controlling costs by restricting treatment to those with fibrosis stage 2 or greater disease was cost ineffective for any patient type compared with treating all patients.
Treatment strategies using interferon-free therapies to treat all HCV-infected persons are cost effective, but short-term cost is high. Among noncirrhotic patients, using the least costly interferon-free regimen, even if it is not single tablet or once daily, is the cost-control strategy that results in best outcomes. Restricting treatment to patients with more advanced disease often results in worse outcomes than treating all patients, and it is not preferred.
用于治疗丙型肝炎病毒(HCV)1型的无干扰素方案有效但成本高昂。目前,美国的医保支付方采用多种策略来控制成本,包括(1)仅对患有晚期疾病的患者进行治疗,以及(2)通过谈判价格折扣以换取独家使用权。
我们使用蒙特卡洛模拟来研究这些治疗政策的预算影响和成本效益,并确定在可及性与成本控制之间取得平衡的策略。结果包括每10000名HCV感染患者的5年未贴现医保支付方成本以及增量成本效益比。
我们发现HCV治疗的预算影响很高,根据治疗方案的选择,每10000名HCV感染患者的5年未贴现成本在10亿美元至23亿美元之间。在非肝硬化患者中,使用成本最低的无干扰素方案可使医保支付方成本降至最低,临床结果差异可忽略不计,即使成本较低的方案便利性和/或有效性较差。在肝硬化患者中,更有效但成本更高的方案仍然具有成本效益。与治疗所有患者相比,将治疗限制在纤维化2期或更严重疾病的患者中以控制成本,对任何患者类型而言都是成本无效的。
使用无干扰素疗法治疗所有HCV感染者的治疗策略具有成本效益,但短期成本较高。在非肝硬化患者中,使用成本最低的无干扰素方案,即使不是单片剂或每日一次给药,也是能带来最佳结果的成本控制策略。将治疗限制在疾病更严重的患者中往往会导致比治疗所有患者更差的结果,因此并非首选策略。