Chest Research Foundation, Marigold Premises, Kalyani Nagar, Pune, 411014, India.
NPJ Prim Care Respir Med. 2017 May 9;27(1):32. doi: 10.1038/s41533-017-0036-8.
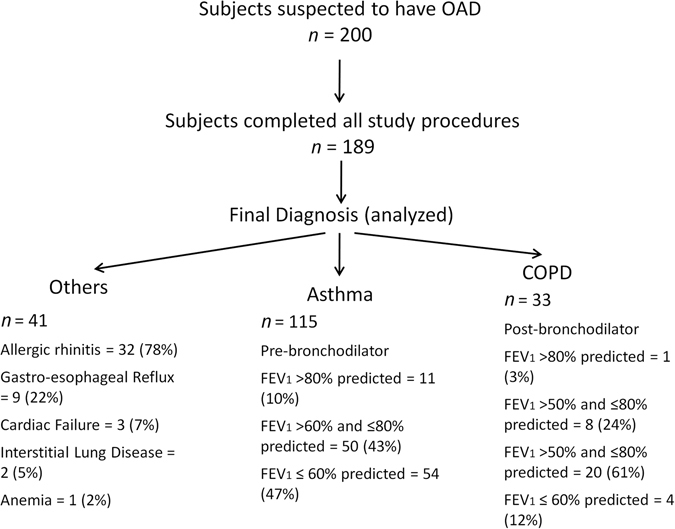
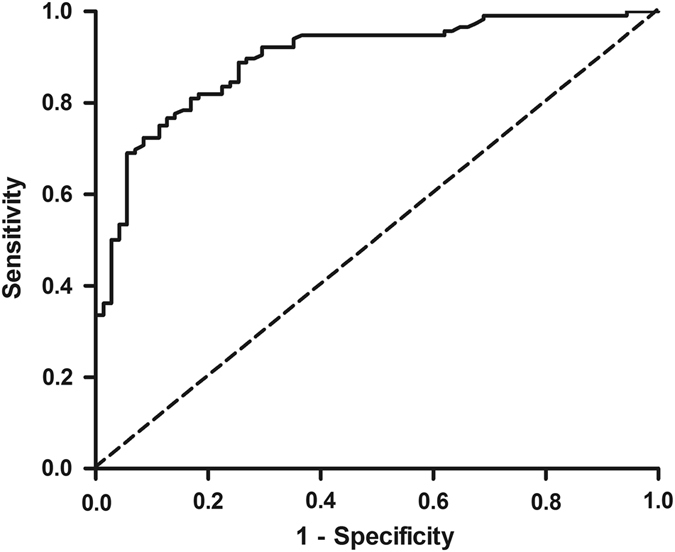
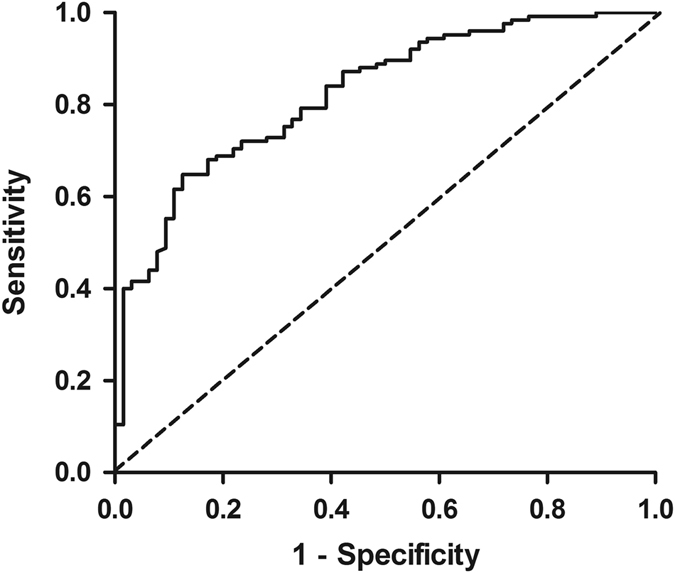
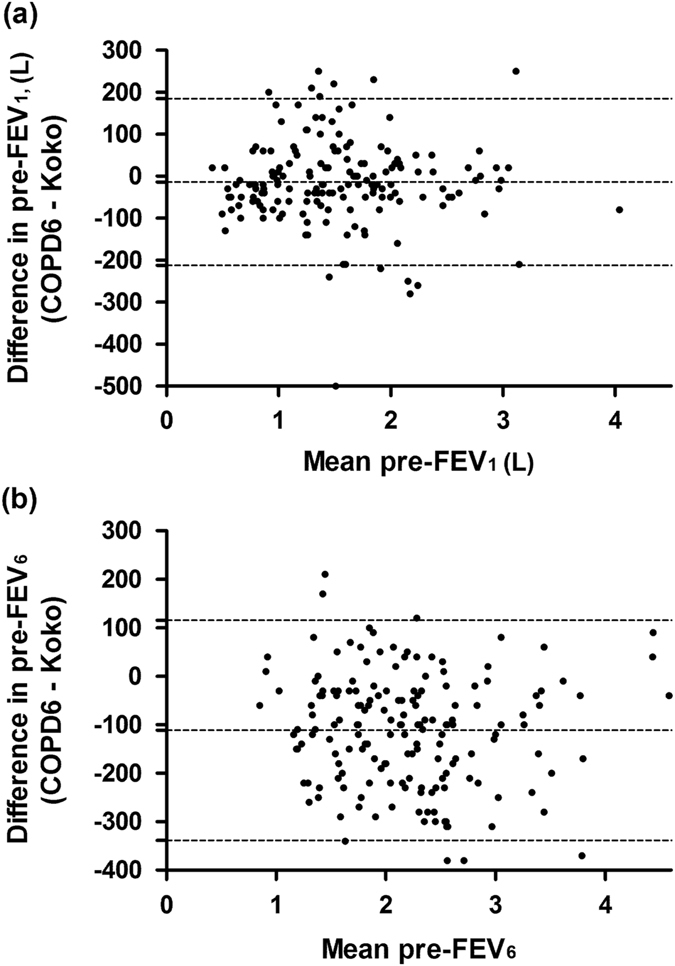
Peak flow meter with questionnaire and mini-spirometer are considered as alternative tools to spirometry for screening of asthma and chronic obstructive pulmonary disease. However, the accuracy of these tools together, in clinical settings for disease diagnosis, has not been studied. Two hundred consecutive patients with respiratory complaints answered a short symptom questionnaire and performed peak expiratory flow measurements, standard spirometry with Koko spirometer and mini-spirometry (COPD-6). Spirometry was repeated after bronchodilation. Physician made a final diagnosis of asthma, chronic obstructive pulmonary disease and others. One eighty nine patients (78 females) with age 51 ± 17 years with asthma (115), chronic obstructive pulmonary disease (33) and others (41) completed the study. "Breathlessness > 6months" and "cough > 6months" were important symptoms to detect obstructive airways disease. "Asymptomatic period > 2 weeks" had the best sensitivity (Sn) and specificity (Sp) to differentiate asthma and chronic obstructive pulmonary disease. A peak expiratory flow of < 80% predicted was the best cut-off to detect airflow limitation (Sn 90%, Sp 50%). Respiratory symptoms with PEF < 80% predicted, had Sn 84 and Sp 93% to detect OAD. COPD-6 device under-estimated FEV by 13 mL (95% CI: -212, 185). At a cut-off of 0.75, the FEV/FEV had the best accuracy (Sn 80%, Sp 86%) to detect airflow limitation. Peak flow meter with few symptom questions can be effectively used in clinical practice for objective detection of asthma and chronic obstructive pulmonary disease, in the absence of good quality spirometry. Mini-spirometers are useful in detection of obstructive airways diseases but FEV measured is inaccurate.
DIFFERENTIATING CONDITIONS IN POORLY-EQUIPPED SETTINGS: A simple questionnaire and peak flow meter measurements can help doctors differentiate between asthma and chronic lung disease. In clinical settings where access to specialist equipment and knowledge is limited, it can be challenging for doctors to tell the difference between asthma and chronic obstructive pulmonary disease (COPD). To determine a viable alternative method for differentiating between these diseases, Rahul Kodgule and colleagues at the Chest Research Foundation in Pune, India, trialed a simplified version of two existing symptom questionnaires, combined with peak flow meter measurements. They assessed 189 patients using this method, and found it aided diagnosis with high sensitivity and specificity. Breathlessness, cough and wheeze were the minimal symptoms required for COPD diagnosis, while the length of asymptomatic periods was most helpful in distinguishing asthma from COPD.
未加说明的内容:峰值流量计与问卷和迷你肺活量计被认为是用于筛查哮喘和慢性阻塞性肺疾病的替代肺功能检测方法。然而,这些工具在临床环境下联合用于疾病诊断的准确性尚未得到研究。200 名有呼吸系统症状的连续患者回答了一个简短的症状问卷,并进行了峰值呼气流量测量、使用 Koko 肺功能仪的标准肺功能检查和迷你肺活量计(COPD-6)检查。支气管扩张后重复肺功能检查。医生根据症状做出哮喘、慢性阻塞性肺病和其他疾病的最终诊断。189 名患者(78 名女性)年龄 51±17 岁,包括哮喘患者 115 名、慢性阻塞性肺病患者 33 名和其他疾病患者 41 名,完成了这项研究。“呼吸困难持续时间>6 个月”和“咳嗽持续时间>6 个月”是检测气道阻塞性疾病的重要症状。“无症状期>2 周”对区分哮喘和慢性阻塞性肺病具有最佳的敏感性(Sn)和特异性(Sp)。呼气峰流量<80%预计值是检测气流受限的最佳截断值(Sn90%,Sp50%)。呼吸症状与 PEF<80%预计值时,对检测 OAD 的 Sn 为 84%,Sp 为 93%。COPD-6 设备低估了 FEV 13mL(95%CI:-212,185)。当截断值为 0.75 时,FEV/FEV 具有最佳的准确性(Sn80%,Sp86%)来检测气流受限。仅使用几个症状问题的峰值流量计可以在没有良好质量的肺功能检查的情况下,在临床实践中有效地用于哮喘和慢性阻塞性肺病的客观检测。迷你肺活量计可用于检测气道阻塞性疾病,但测量的 FEV 不准确。
慢性肺病:在资源匮乏的环境下区分不同病症:一个简单的问卷和峰值流量计测量可以帮助医生区分哮喘和慢性肺病。在设备和知识获取有限的临床环境中,医生很难区分哮喘和慢性阻塞性肺疾病(COPD)。为了确定一种可行的替代方法来区分这些疾病,印度浦那 Chest Research Foundation 的 Rahul Kodgule 及其同事试验了两种现有症状问卷的简化版本,结合峰值流量计测量。他们使用这种方法评估了 189 名患者,发现该方法具有很高的敏感性和特异性,有助于诊断。呼吸困难、咳嗽和喘息是 COPD 诊断所需的最低限度症状,而无症状期的长短对区分哮喘和 COPD 最有帮助。