Liu Vincent X, Rosas Efren, Hwang Judith, Cain Eric, Foss-Durant Anne, Clopp Molly, Huang Mengfei, Lee Derrick C, Mustille Alex, Kipnis Patricia, Parodi Stephen
Division of Research, Kaiser Permanente, Oakland, California2The Permanente Medical Group, Oakland, California.
The Permanente Medical Group, Oakland, California.
JAMA Surg. 2017 Jul 19;152(7):e171032. doi: 10.1001/jamasurg.2017.1032.
Novel approaches to perioperative surgical care focus on optimizing nutrition, mobility, and pain management to minimize adverse events after surgical procedures.
To evaluate the outcomes of an enhanced recovery after surgery (ERAS) program among 2 target populations: patients undergoing elective colorectal resection and patients undergoing emergency hip fracture repair.
DESIGN, SETTING, AND PARTICIPANTS: A pre-post difference-in-differences study before and after ERAS implementation in the target populations compared with contemporaneous surgical comparator groups (patients undergoing elective gastrointestinal surgery and emergency orthopedic surgery). Implementation began in February and March 2014 and concluded by the end of 2014 at 20 medical centers within the Kaiser Permanente Northern California integrated health care delivery system.
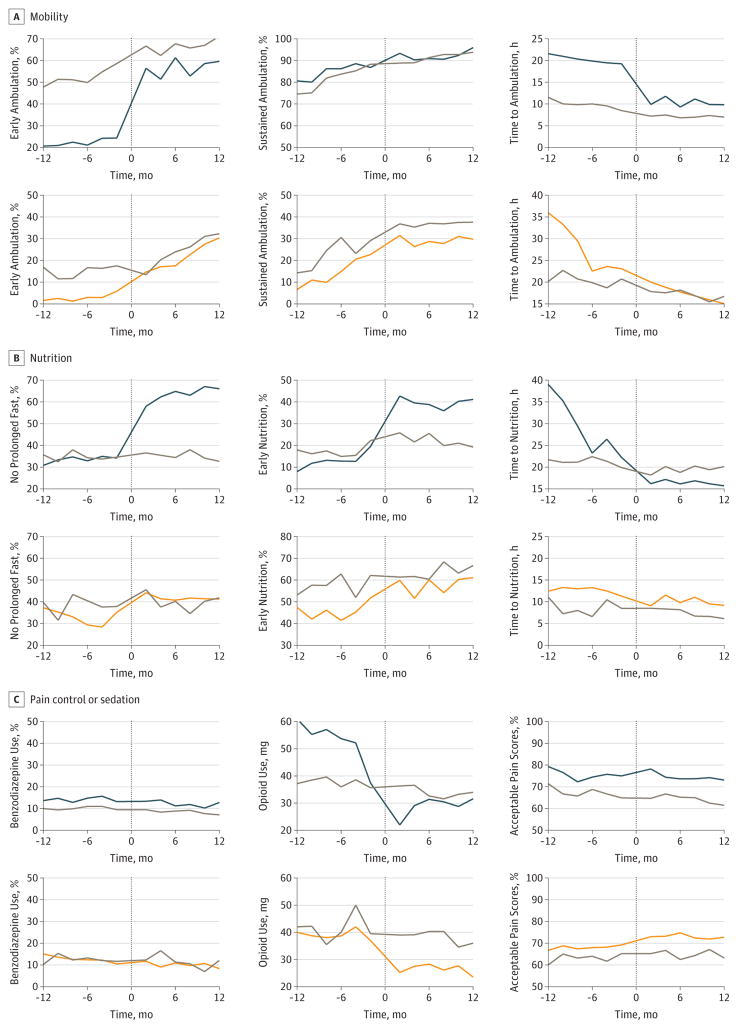
A multifaceted ERAS program designed with a particular focus on perioperative pain management, mobility, nutrition, and patient engagement.
The primary outcome was hospital length of stay. Secondary outcomes included hospital mortality, home discharge, 30-day readmission rates, and complication rates.
The study included a total of 3768 patients undergoing elective colorectal resection (mean [SD] age, 62.7 [14.1] years; 1812 [48.1%] male) and 5002 patients undergoing emergency hip fracture repair (mean [SD] age, 79.5 [11.8] years; 1586 [31.7%] male). Comparator surgical patients included 5556 patients undergoing elective gastrointestinal surgery and 1523 patients undergoing emergency orthopedic surgery. Most process metrics had significantly greater changes in the ERAS target populations after implementation compared with comparator surgical populations, including those for ambulation, nutrition, and opioid use. Hospital length of stay and postoperative complication rates were also significantly lower among ERAS target populations after implementation. The rate ratios for postoperative complications were 0.68 (95% CI, 0.46-0.99; P = .04) for patients undergoing colorectal resection and 0.67 (95% CI, 0.45-0.99, P = .05) for patients with hip fracture. Among patients undergoing colorectal resection, ERAS implementation was associated with decreased rates of hospital mortality (0.17; 95% CI, 0.03-0.86; P = .03), whereas among patients with hip fracture, implementation was associated with increased rates of home discharge (1.24; 95% CI, 1.06-1.44; P = .007).
Multicenter implementation of an ERAS program among patients undergoing elective colorectal resection and patients undergoing emergency hip fracture repair successfully altered processes of care and was associated with significant absolute and relative decreases in hospital length of stay and postoperative complication rates. Rapid, large-scale implementation of a multidisciplinary ERAS program is feasible and effective in improving surgical outcomes.
围手术期外科护理的新方法侧重于优化营养、活动能力和疼痛管理,以尽量减少手术后的不良事件。
评估手术加速康复(ERAS)计划在2个目标人群中的效果:接受择期结直肠切除术的患者和接受急诊髋部骨折修复术的患者。
设计、设置和参与者:在目标人群中实施ERAS前后进行的一项前后差异研究,并与同期手术对照人群(接受择期胃肠手术和急诊骨科手术的患者)进行比较。实施工作于2014年2月和3月开始,并于2014年底在北加利福尼亚凯撒永久医疗综合医疗服务系统内的20个医疗中心完成。
一个多方面的ERAS计划,特别关注围手术期疼痛管理、活动能力、营养和患者参与度。
主要结局是住院时间。次要结局包括医院死亡率、出院回家、30天再入院率和并发症发生率。
该研究共纳入3768例接受择期结直肠切除术的患者(平均[标准差]年龄,62.7[14.1]岁;1812例[48.1%]为男性)和5002例接受急诊髋部骨折修复术的患者(平均[标准差]年龄,79.5[11.8]岁;1586例[31.7%]为男性)。对照手术患者包括5556例接受择期胃肠手术的患者和1523例接受急诊骨科手术的患者。与对照手术人群相比,大多数过程指标在实施ERAS后在目标人群中的变化显著更大,包括行走、营养和阿片类药物使用方面的指标。实施ERAS后,目标人群的住院时间和术后并发症发生率也显著降低。接受结直肠切除术患者术后并发症发生率的比值比为0.68(95%CI,0.46-0.99;P = 0.04),髋部骨折患者为0.67(95%CI,0.45-0.99,P = 0.05)。在接受结直肠切除术的患者中,ERAS的实施与医院死亡率降低相关(0.17;95%CI,0.03-0.86;P = 0.03),而在髋部骨折患者中,实施与出院回家率增加相关(1.24;95%CI,1.06-1.44;P = 0.007)。
在接受择期结直肠切除术的患者和接受急诊髋部骨折修复术的患者中多中心实施ERAS计划成功改变了护理流程,并与住院时间和术后并发症发生率的显著绝对和相对降低相关。快速、大规模实施多学科ERAS计划在改善手术结局方面是可行且有效的。