Collins Denis, Jacob Wolfgang, Cejalvo Juan Miguel, Ceppi Maurizio, James Ian, Hasmann Max, Crown John, Cervantes Andrés, Weisser Martin, Bossenmaier Birgit
National Institute for Cellular Biotechnology, Dublin City University, Dublin, Ireland.
Roche Innovation Center Munich, Penzberg, Germany.
PLoS One. 2017 May 11;12(5):e0177331. doi: 10.1371/journal.pone.0177331. eCollection 2017.
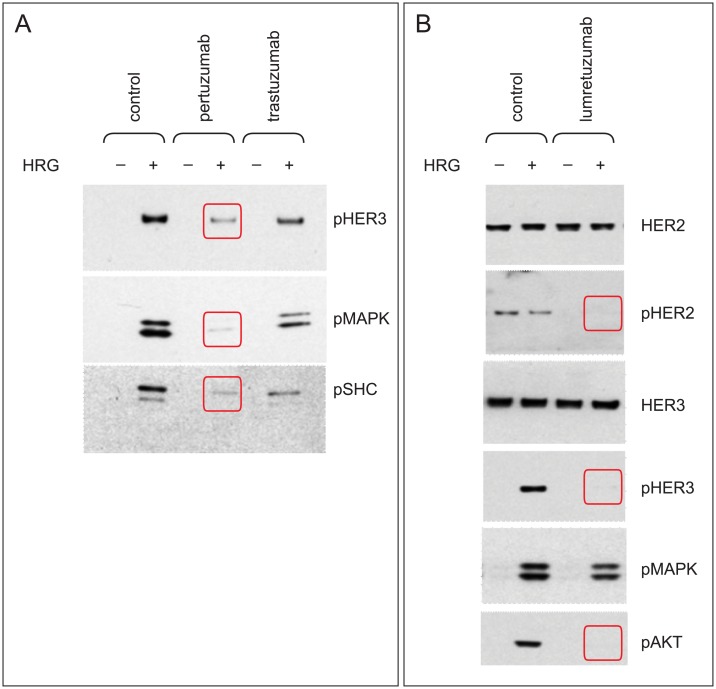
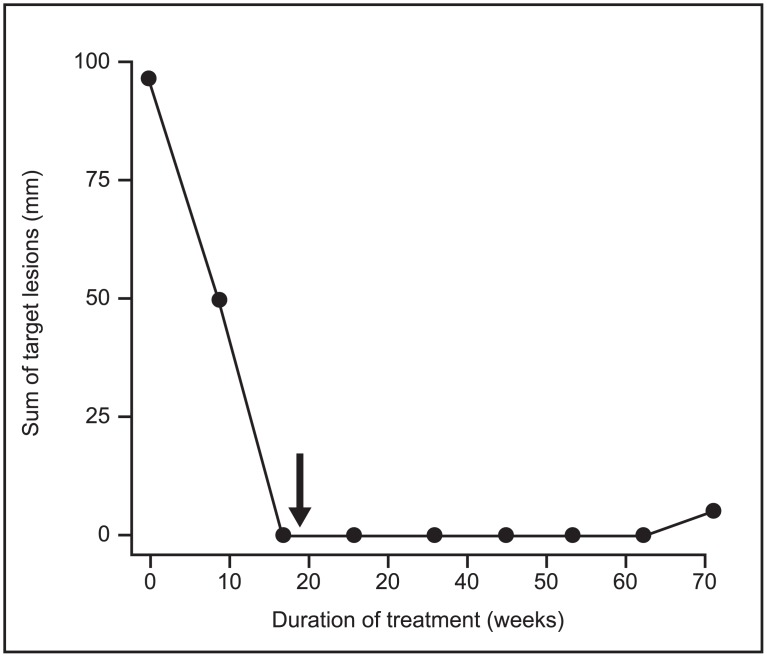
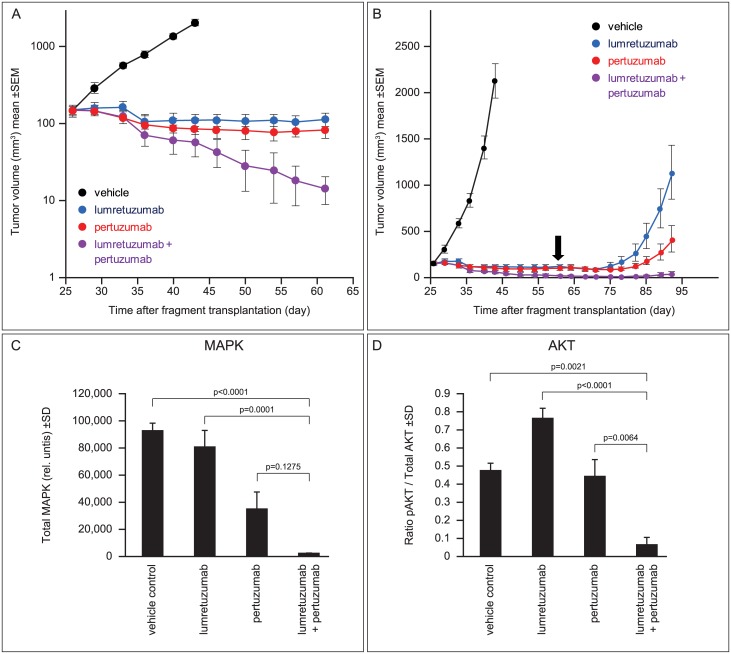
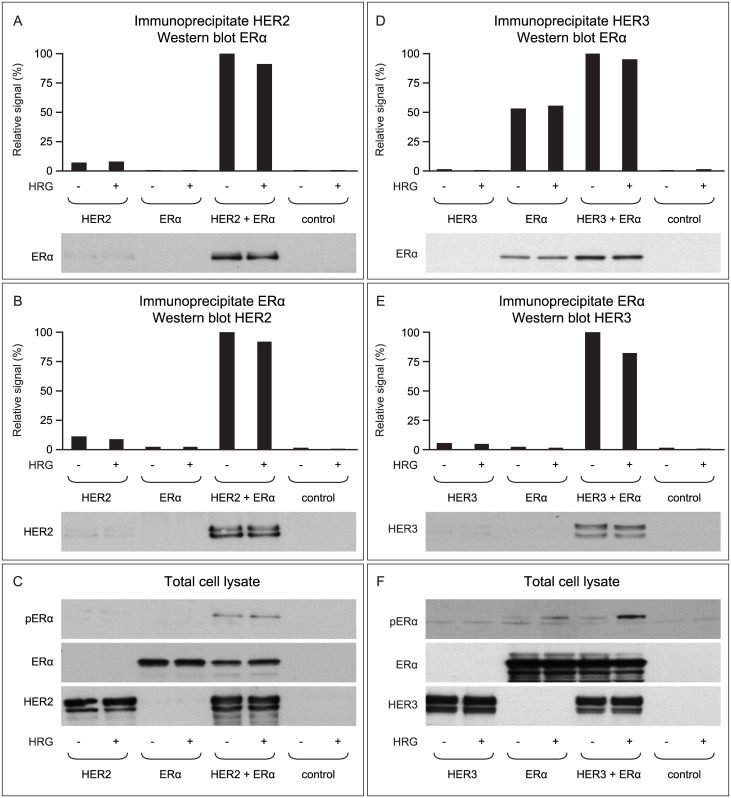
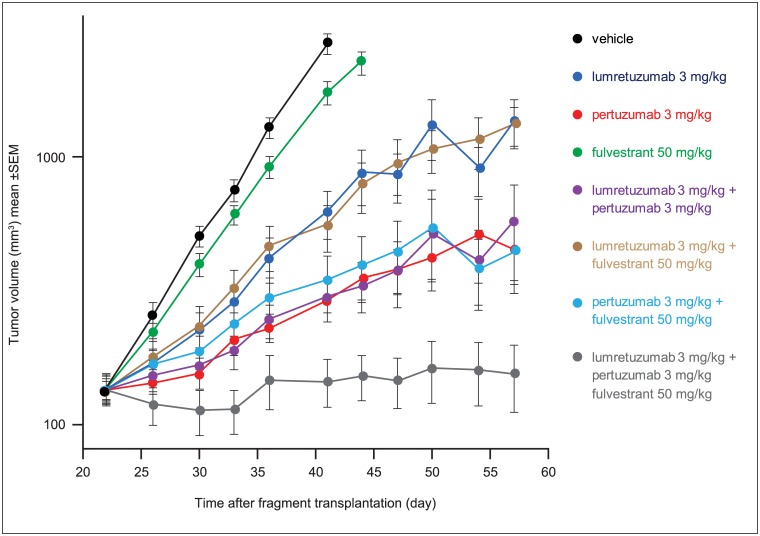
Bidirectional cross talk between members of the human epidermal growth factor family of receptors (HER) and the estrogen receptor (ER) is believed to underlie resistance mechanisms that develop in response to treatment with anti-HER agents and endocrine therapy. We investigated the interaction between HER2, HER3 and the ER in vitro using human embryonic kidney cells transfected with human HER2, HER3, and ERα. We also investigated the additive efficacy of combination regimens consisting of anti-HER3 (lumretuzumab), anti-HER2 (pertuzumab), and endocrine (fulvestrant) therapy in vivo. Our data show that both HER2 and HER3 can directly complex with the ER and can mediate phosphorylation of the ER. Phosphorylation of the ER was only observed in cells that expressed both HER2 and ERα or in heregulin-stimulated cells that expressed both HER3 and ERα. Using a mouse xenograft model of ER+/HER2-low (HER2 immunohistochemistry 1+ or 2+ without gene amplification) human breast cancer we show that the combination of lumretuzumab and pertuzumab is highly efficacious and induces long-lasting tumor regression in vivo and adding endocrine therapy (fulvestrant) to this combination further improved efficacy. In addition, a prolonged clinical response was observed with the combination of lumretuzumab and pertuzumab in a patient with ER+/HER2-low breast cancer who had failed endocrine therapy. These preclinical data confirm that direct cross talk exists between HER2/HER3 and ER which may explain the resistance mechanisms to endocrine therapy and monoclonal antibodies that target HER2 and HER3. Our data also indicate that the triplet of anti-HER2, anti-HER3, and endocrine therapy might be an efficacious combination for treating patients with ER+/HER2-low breast cancer, which is an area of significant unmet medical need.
人表皮生长因子受体(HER)家族成员与雌激素受体(ER)之间的双向串扰被认为是对抗HER药物和内分泌治疗产生耐药机制的基础。我们使用转染了人HER2、HER3和ERα的人胚肾细胞在体外研究了HER2、HER3与ER之间的相互作用。我们还在体内研究了由抗HER3(鲁美替尼单抗)、抗HER2(帕妥珠单抗)和内分泌(氟维司群)治疗组成的联合方案的附加疗效。我们的数据表明,HER2和HER3都可以直接与ER形成复合物,并可以介导ER的磷酸化。仅在同时表达HER2和ERα的细胞中或在同时表达HER3和ERα的这里替尼刺激的细胞中观察到ER的磷酸化。使用ER + /HER2低(HER2免疫组化1 +或2 +且无基因扩增)人乳腺癌的小鼠异种移植模型,我们表明鲁美替尼单抗和帕妥珠单抗的联合治疗非常有效,并在体内诱导持久的肿瘤消退,在此联合治疗中加入内分泌治疗(氟维司群)可进一步提高疗效。此外,在一名内分泌治疗失败的ER + /HER2低乳腺癌患者中,观察到鲁美替尼单抗和帕妥珠单抗联合治疗产生了延长的临床反应。这些临床前数据证实HER2/HER3与ER之间存在直接串扰,这可能解释了对内分泌治疗以及靶向HER2和HER3的单克隆抗体的耐药机制。我们的数据还表明,抗HER2、抗HER3和内分泌治疗三联疗法可能是治疗ER + /HER2低乳腺癌患者的有效联合方案,这是一个存在重大未满足医疗需求的领域。