Loubet Paul, Voiriot Guillaume, Houhou-Fidouh Nadhira, Neuville Mathilde, Bouadma Lila, Lescure Francois-Xavier, Descamps Diane, Timsit Jean-François, Yazdanpanah Yazdan, Visseaux Benoit
IAME, UMR 1137, INSERM, Université Paris Diderot, Sorbonne Paris Cité, Service de Maladies Infectieuses et Tropicales, Hôpital Bichat, AP-HP, Paris, France.
AP-HP, Hôpital Bichat-Claude Bernard, Service de réanimation médicale et infectieuse, F-75018 Paris, France.
J Clin Virol. 2017 Jun;91:52-57. doi: 10.1016/j.jcv.2017.04.001. Epub 2017 Apr 22.
Data on the frequency and role of respiratory viruses (RVs) in hospital-acquired pneumonia (HAP) are still scarce.
We assessed the proportion of RVs and their impact on the outcome of hospital-acquired pneumonia (HAP) in the intensive care unit (ICU).
Cases of HAP were retrospectively selected among patients who underwent screening for RVs by multiplex PCR (mPCR) in the ICU of a French tertiary care hospital from May 2014 to April 2016. ICU length of stay and in-hospital mortality were compared between four groups defined according to the identified pathogens: virus only (V), virus/bacteria (V/B), bacteria only (B) and no pathogen (Neg). When available, previous mPCR was retrieved in order to assess possible chronic viral carriage.
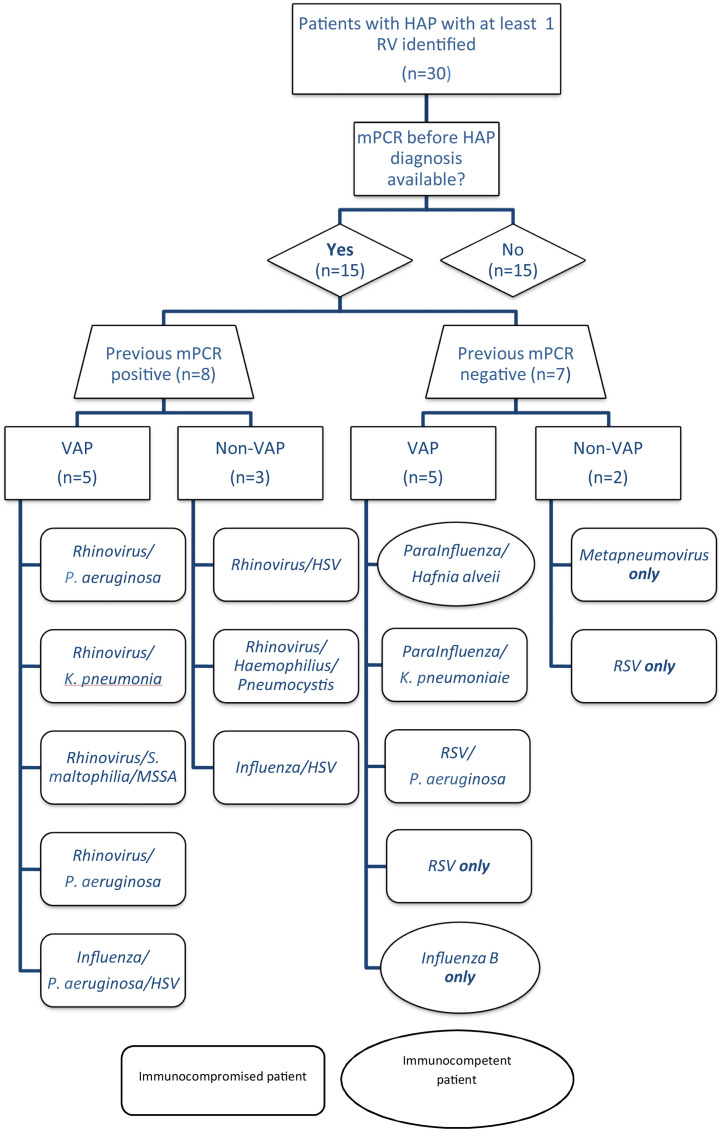
Overall, 95/999 (10%) ICU patients who underwent mPCR had HAP (V(17,18%), V/B(13,14%), B(60,63%), Neg(5,5%)). Median age was 61 years and 45 (47%) were immunocompromised. Influenza (27%) and rhinovirus (27%) were the most common RVs. V/B group had higher mortality rate than B and V groups (62% vs. 40% and 35%, p=0.3) and a significantly longer length of stay (31days (18-48)) than V group (5days (3-11), p=0.0002)) and B group (14.5days (5.5-25.5), p=0.007)). Among the 15 patients with available mPCR tests before viral HAP, seven were negative and eight were positive corresponding to long-term carriage of community-acquired viruses.
RVs were detected in 32% of HAP patients who underwent mPCR. Two situations were encountered: (i) acute acquired viral infection; (ii) long-term viral carriage (mostly rhinovirus) especially in immunocompromised patients complicated by a virus/bacteria coinfection. The latter was associated with a longer length of stay and a trend toward a higher mortality.
关于呼吸道病毒(RVs)在医院获得性肺炎(HAP)中的频率和作用的数据仍然很少。
我们评估了重症监护病房(ICU)中RVs的比例及其对医院获得性肺炎(HAP)结局的影响。
回顾性选择2014年5月至2016年4月在法国一家三级护理医院ICU中接受多重PCR(mPCR)筛查RVs的患者中的HAP病例。根据鉴定出的病原体将患者分为四组:仅病毒组(V)、病毒/细菌组(V/B)、仅细菌组(B)和无病原体组(Neg),比较各组的ICU住院时间和院内死亡率。如有可用的先前mPCR检测结果,则进行检索以评估可能的慢性病毒携带情况。
总体而言,999例接受mPCR检测的ICU患者中有95例(10%)发生HAP(V组(17例,18%)、V/B组(13例,14%)、B组(60例,63%)、Neg组(5例,5%))。中位年龄为61岁,45例(47%)为免疫功能低下患者。流感病毒(27%)和鼻病毒(27%)是最常见的RVs。V/B组的死亡率高于B组和V组(62%对40%和35%,p = 0.3),住院时间明显长于V组(5天(3 - 11天),p = 0.0002))和B组(14.5天(5.5 - 25.5天),p = 0.007))。在15例病毒感染性HAP发生前有可用mPCR检测结果的患者中,7例为阴性,8例为阳性,对应社区获得性病毒的长期携带。
在接受mPCR检测的HAP患者中,32%检测到RVs。遇到两种情况:(i)急性获得性病毒感染;(ii)长期病毒携带(主要是鼻病毒),尤其是在合并病毒/细菌混合感染且免疫功能低下的患者中。后者与更长的住院时间和更高的死亡率趋势相关。