Demir Semra, Gelincik Asli, Akdeniz Nilgun, Aktas-Cetin Esin, Olgac Muge, Unal Derya, Ertek Belkis, Coskun Raif, Colakoğlu Bahattin, Deniz Gunnur, Buyukozturk Suna
Division of Immunology and Allergic Diseases, Department of Internal Medicine, Istanbul University, Istanbul Faculty of Medicine, Istanbul, Turkey.
Department of Immunology, Institute of Experimental Medicine (DETAE), Istanbul University, Istanbul, Turkey.
Allergy Asthma Immunol Res. 2017 Jul;9(4):347-359. doi: 10.4168/aair.2017.9.4.347.
Reports evaluating diagnosis and cross reactivity of quinolone hypersensitivity have revealed contradictory results. Furthermore, there are no reports investigating the cross-reactivity between gemifloxacin (GFX) and the others. We aimed to detect the usefulness of diagnostic tests of hypersensitivity reactions to quinolones and to evaluate the cross reactivity between different quinolones including the latest quinolone GFX.
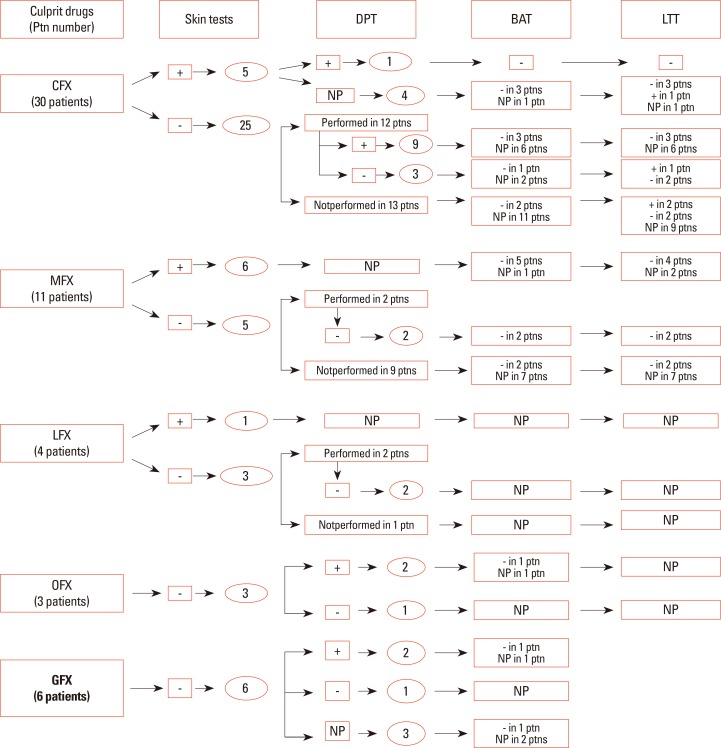
We studied 54 patients (mean age 42.31±10.39 years; 47 female) with 57 hypersensitivity reactions due to different quinolones and 10 nonatopic quinolone tolerable control subjects. A detailed clinical history, skin test (ST), and single-blind placebo-controlled drug provocation test (SBPCDPT), as well as basophil activation test (BAT) and lymphocyte transformation test (LTT) were performed with the culprit and alternative quinolones including ciprofloxacin (CFX), moxifloxacin (MFX), levofloxacin (LFX), ofloxacin (OFX), and GFX.
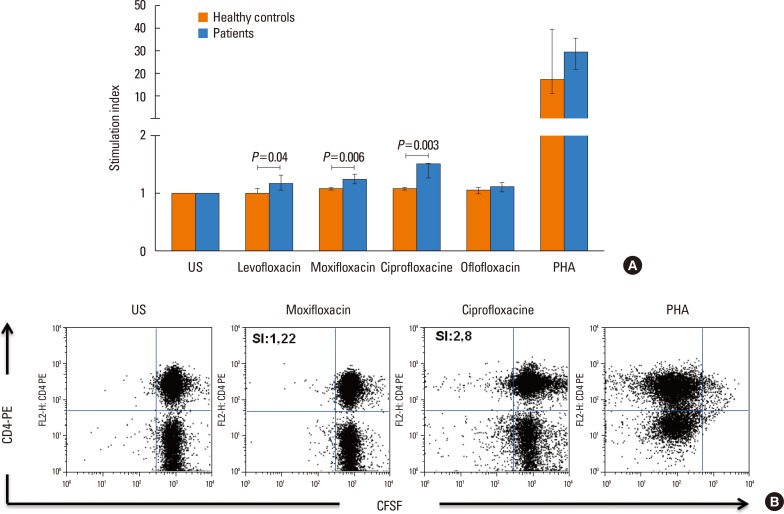
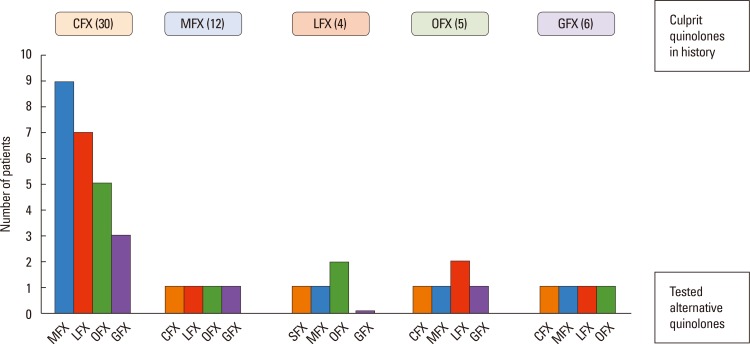
The majority (75.9%) of the patients reported immediate type reactions to various quinolones. The most common culprit drug was CFX (52.6%) and the most common reaction type was urticaria (26.3%). A quarter of the patients (24.1%) reacted to SBPCDPTs, although their STs were negative; while false ST positivity was 3.5% and ST/SBPCDPTs concordance was only 1.8%. Both BAT and LTT were not found useful in quinolone hypersensitivity. Cross-reactivity was primarily observed between LFX and OFX (50.0%), whereas it was the least between MFX and the others, and in GFX hypersensitive patients the degree of cross-reactivity to the other quinolones was 16.7%.
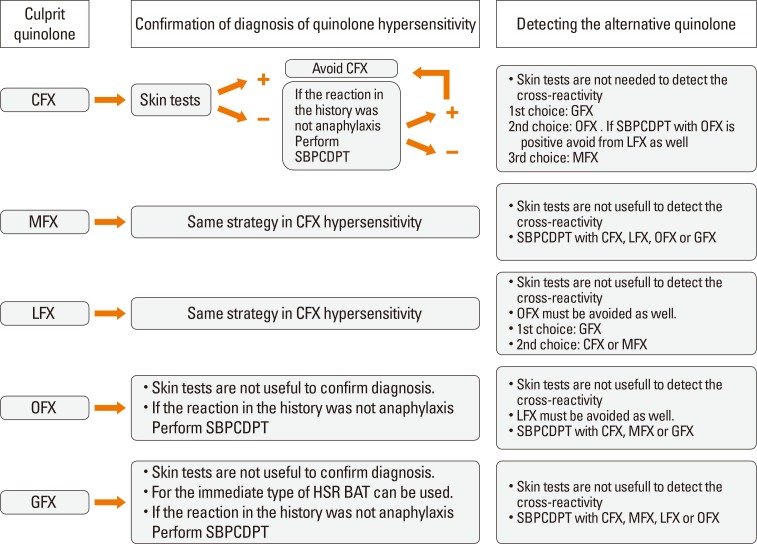
These results suggest that STs, BAT, and LTT are not supportive in the diagnosis of a hypersensitivity reaction to quinolone as well as in the prediction of cross-reactivity. Drug provocation tests (DPTs) are necessary to identify both culprit and alternative quinolones.
评估喹诺酮超敏反应诊断及交叉反应性的报告结果相互矛盾。此外,尚无关于吉米沙星(GFX)与其他喹诺酮类药物之间交叉反应性的研究报告。我们旨在检测喹诺酮类药物超敏反应诊断试验的有效性,并评估包括最新喹诺酮类药物GFX在内的不同喹诺酮类药物之间的交叉反应性。
我们研究了54例因不同喹诺酮类药物发生57次超敏反应的患者(平均年龄42.31±10.39岁;女性47例)以及10例非特应性且对喹诺酮类药物耐受的对照受试者。对包括环丙沙星(CFX)、莫西沙星(MFX)、左氧氟沙星(LFX)、氧氟沙星(OFX)和GFX在内的致病及替代喹诺酮类药物进行了详细的临床病史、皮肤试验(ST)、单盲安慰剂对照药物激发试验(SBPCDPT),以及嗜碱性粒细胞活化试验(BAT)和淋巴细胞转化试验(LTT)。
大多数患者(75.9%)报告对各种喹诺酮类药物有速发型反应。最常见的致病药物是CFX(52.6%),最常见的反应类型是荨麻疹(26.3%)。四分之一的患者(24.1%)对SBPCDPT有反应,尽管其ST结果为阴性;而ST假阳性率为3.5%,ST/SBPCDPT的一致性仅为1.8%。未发现BAT和LTT对喹诺酮超敏反应有诊断价值。交叉反应性主要见于LFX和OFX之间(50.0%),而MFX与其他药物之间的交叉反应性最低,在GFX超敏患者中,对其他喹诺酮类药物的交叉反应程度为16.7%。
这些结果表明,ST、BAT和LTT在喹诺酮类药物超敏反应的诊断以及交叉反应性预测方面均无支持作用。药物激发试验(DPT)对于确定致病及替代喹诺酮类药物是必要的。