Mauriello Alessandro, Rovella Valentina, Borri Filippo, Anemona Lucia, Giannini Elena, Giacobbi Erica, Saggini Andrea, Palmieri Giampiero, Anselmo Alessandro, Bove Pierluigi, Melino Gerry, Valentina Guardini, Tesauro Manfredi, Gabriele D'Urso, Di Daniele Nicola
Anatomic Pathology, Department of Experimental Medicine and Surgery, Tor Vergata University, Rome, Italy.
Hypertension and Nephrology Unit, Department of Systems Medicine, Tor Vergata University, Rome, Italy.
Nephrol Dial Transplant. 2017 Jun 1;32(6):1053-1060. doi: 10.1093/ndt/gfx069.
BACKGROUND.: Normalization of arterial pressure occurs in just a few patients with hypertensive chronic kidney disease undergoing kidney transplantation. Hypertension in kidney transplant recipients may be related to multiple factors. We aimed to assess whether hypertension in kidney-transplanted patients may be linked to reinnervation of renal arteries of the transplanted kidney.
METHODS.: We investigated renal arteries innervation from native and transplanted kidneys in three patients 5 months, 2 years and 11 years after transplantation, respectively. Four transplanted kidneys from non-hypertensive patients on immunosuppressive treatment without evidence of hypertensive arteriolar damage were used as controls.
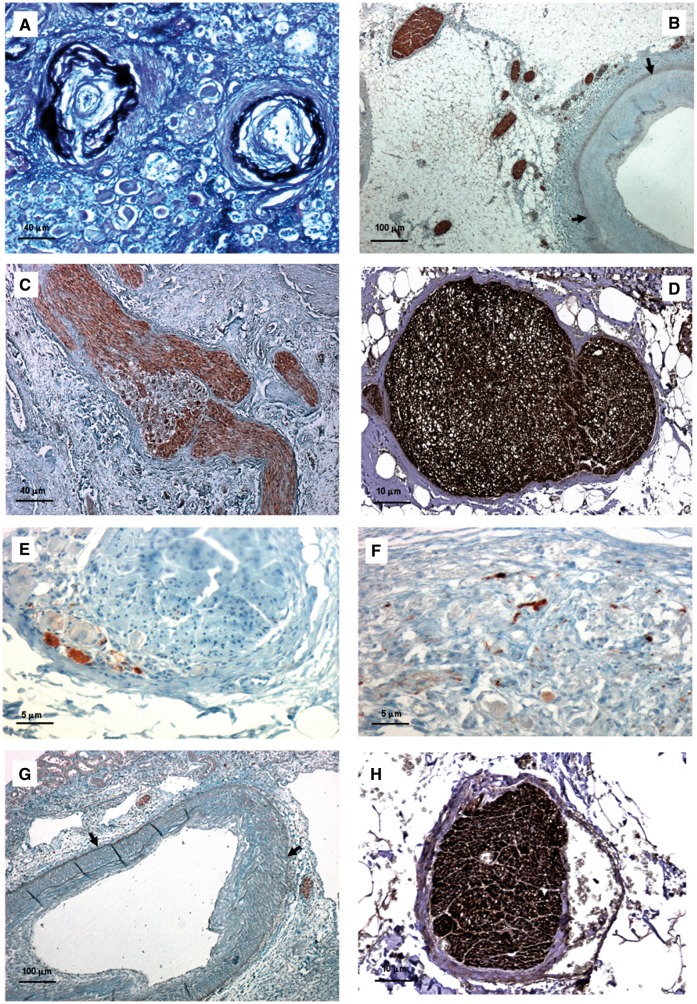
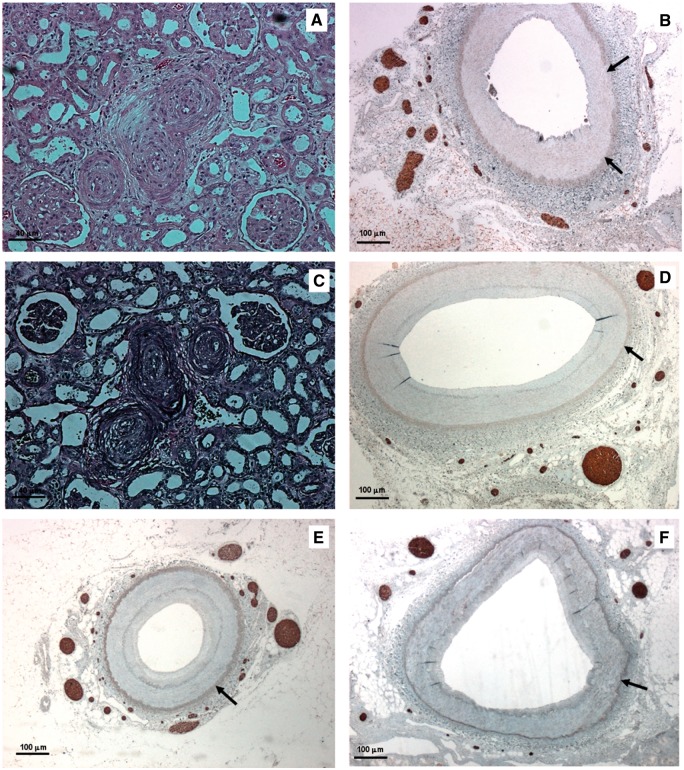
. Evidence of nerve sprouting was observed as early as 5 months following transplantation, probably originated from ganglions of recipient patient located near the arterial anastomosis and was associated with mild hypertensive arteriolar damage. Regeneration of periadventitial nerves was already complete 2 years after transplantation. Nerve density tended to reach values observed in native kidney arteries and was associated with hypertension-related arteriolar lesions in transplanted kidneys. Control kidneys, albeit on an immunosuppressive regimen, presented only a modest regeneration of sympathetic nerves.
. Our results suggest that the considerable increase in sympathetic nerves, as found in patients with severe arterial damage, may be correlated to hypertension rather than to immunosuppressive therapy, thus providing a morphological basis for hypertension recurrence despite renal denervation.
在接受肾移植的高血压慢性肾病患者中,仅有少数患者的动脉血压恢复正常。肾移植受者的高血压可能与多种因素有关。我们旨在评估肾移植患者的高血压是否可能与移植肾肾动脉的神经再支配有关。
我们分别调查了3例患者在移植后5个月、2年和11年时来自自体肾和移植肾的肾动脉神经支配情况。将4例接受免疫抑制治疗且无高血压小动脉损伤证据的非高血压患者的移植肾用作对照。
早在移植后5个月就观察到神经发芽的证据,可能起源于位于动脉吻合口附近的受者神经节,并与轻度高血压小动脉损伤有关。移植后2年外膜周围神经的再生已经完成。神经密度趋于达到在自体肾动脉中观察到的值,并与移植肾中与高血压相关的小动脉病变有关。对照肾尽管接受免疫抑制治疗,但仅出现了适度的交感神经再生。
我们的结果表明,在严重动脉损伤患者中发现的交感神经显著增加可能与高血压有关,而非与免疫抑制治疗有关,从而为尽管进行了肾去神经支配但高血压仍复发提供了形态学基础。