Zhao Jianxi, Ren Gang, Cai Rong, Chen Jian, Li Huali, Guo Chen, He Wenguang, Wu Xiangru, Zhang Wenjie
Department of Radiology, Xinhua Hospital Affiliated to Shanghai Jiaotong University School of Medicine, Shanghai 200092, China.
Department of Radiotherapy, Ruijin Hospital Affiliated to Shanghai Jiaotong University School of Medicine, Shanghai 200025, China.
Oncotarget. 2017 Jul 11;8(28):45698-45709. doi: 10.18632/oncotarget.17389.
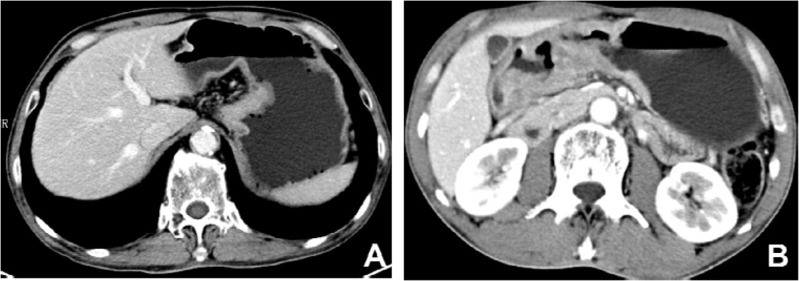
Mucinous gastric carcinoma (MGC) is a rare histological subtype of gastric cancer. The clinicopathological characteristics and CT features of MGC remain controversial. This study aimed to determine the clinicopathological characteristics and CT features of MGC. We reviewed 62 patients with MGC and 104 patients with non-mucinous gastric carcinoma (NMGC), pathologically confirmed between 2003 and 2015. There are significant differences in some clinicopathological characteristics and CT features between MGC and NMGC. NMGC occurs preferentially in males and more frequently in the lower third of the stomach. Patients with MGC were characterized by larger tumor size, more advanced tumor stages (II and III) and fewer lymphatic invasions. Layered enhancement (83.3%) was the main pattern of MGC, while the most common pattern in NMGC was homogeneous enhancement (52.6%), followed by heterogonous enhancement (34.6%). The degree of enhancement of the inner layer in MGC was significantly higher than in NMGC (ΔCT of portal venous phase: 54.57 Hu vs. 47.19 Hu, P = 0.034), while the middle or outer layer in MGC was significantly less enhanced (ΔCT of portal venous phase: 19.07 Hu vs. 33.09 Hu, P <0.001). Calcifications were more common in MGC (P <0.001). ROC curves revealed that the most effective variables in distinguishing MGC and NMGC were ΔCT of the middle or outer layer in the arterial phase (AUC=0.774) and portal venous phase (AUC=0.774), followed by the attenuation value of the middle or outer layer in the unenhanced phase (AUC=0.763). Calcifications had a high specificity (98.7%) in the diagnosis of MGC. The accuracy (86.1%), sensitivity (83.3%) and specificity (87.2%) of layered enhancement in diagnosing MGC were all high. Therefore, MGC was more likely to have larger tumor size and more advanced tumor stage (II and III) than NMGC. The thicker gastric wall, layered enhancement pattern and calcification were highly suggestive CT features for differentiating MGC from NMGC.
黏液性胃癌(MGC)是一种罕见的胃癌组织学亚型。MGC的临床病理特征和CT表现仍存在争议。本研究旨在确定MGC的临床病理特征和CT表现。我们回顾了2003年至2015年间经病理证实的62例MGC患者和104例非黏液性胃癌(NMGC)患者。MGC和NMGC在一些临床病理特征和CT表现上存在显著差异。NMGC好发于男性,且更常见于胃的下三分之一。MGC患者的特点是肿瘤体积较大、肿瘤分期更晚(II期和III期)且淋巴侵犯较少。分层强化(83.3%)是MGC的主要强化方式,而NMGC最常见的强化方式是均匀强化(52.6%),其次是不均匀强化(34.6%)。MGC内层的强化程度明显高于NMGC(门静脉期ΔCT:54.57 Hu对47.19 Hu,P = 0.034),而MGC中层或外层的强化程度明显较低(门静脉期ΔCT:19.07 Hu对33.09 Hu,P <0.001)。钙化在MGC中更常见(P <0.001)。ROC曲线显示,区分MGC和NMGC最有效的变量是动脉期和门静脉期中层或外层的ΔCT(AUC = 0.774),其次是平扫期中层或外层的衰减值(AUC = 0.763)。钙化在MGC诊断中具有较高的特异性(98.7%)。分层强化诊断MGC的准确性(86.1%)、敏感性(83.3%)和特异性(87.2%)均较高。因此,与NMGC相比,MGC更可能具有更大的肿瘤体积和更晚的肿瘤分期(II期和III期)。胃壁增厚、分层强化模式和钙化是鉴别MGC和NMGC的高度提示性CT表现。