Gamst-Jensen Hejdi, Lippert Freddy K, Egerod Ingrid
Emergency Medical Services Copenhagen, University of Copenhagen, Telegrafvej 5, 2. Sal, 2750, Ballerup, Denmark.
Trauma Centre, Rigshospitalet, University of Copenhagen, Blegdamsvej 9, 2100, Copenhagen, Denmark.
Scand J Trauma Resusc Emerg Med. 2017 May 15;25(1):52. doi: 10.1186/s13049-017-0390-0.
Telephone consultation and triage are used to limit the workload on emergency departments. Lack of visual cues and clinical tests put telephone consultations to a disadvantage compared to face-to-face consultations increasing the risk of under-triage. Under-triage occurs in telephone triage; however why under-triage happens is not explored yet. The aim of the study was to describe situations of under-triage in context, to assess the quality of under-triaged calls, and to identify communication patterns contributing to under-triage in a regional OOH service in the capital region of Denmark.
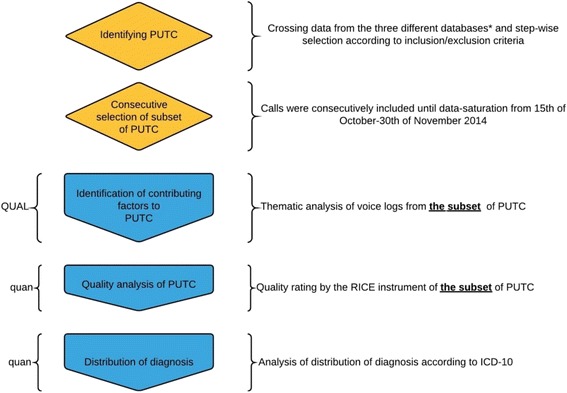
Explanatory simultaneous mixed method with thematic analysis and descriptive statistics was chosen. The study was carried out in an Out-Of-Hours service (OOH) in the Capital Region of Denmark, Copenhagen. Under-triage was defined as Potentially Under-Triaged Calls (PUTC) by specific criteria to an OOH Hotline, and identification by integration of three databases: Medical Hotline database, Emergency number database, including the Ambulance database, and electronic patient records. Distribution of PUTC were carried out using ICD-10 codes to identify diagnosis and main themes identified by qualitative analysis of audio recorded under-triaged calls. Study period was October 15 to November 30 2014.
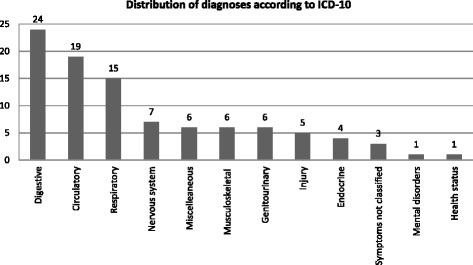
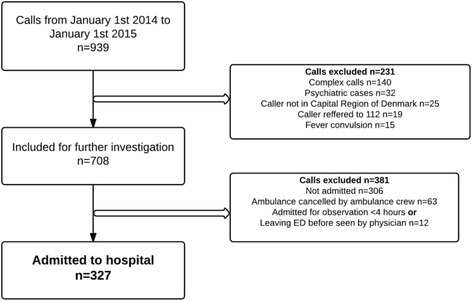
Three hundred twenty seven PUTC were identified, representing 0.04% of all calls (n = 937.056) to the OOH. Distribution of PUTC according to diagnoses was: digestive (24%), circulatory (19%), respiratory (15%) and all others (42%). Thematic analysis of the voice logs suggested that inadequate communication and non-normative symptom description contributed to under-triage.
The incidence of potentially under-triage is low (0.04%). However, the over-representation of digestive, circulatory, and respiratory diagnoses might suggest that under-triage is related to inadequate symptom description. We recommend that caller and call-handler collaborate systematically on problem identification and negotiate non-normative symptom description.
The incidence of under-triage is low (0.04%). However, the over-representation of digestive, circulatory, and respiratory diagnoses might suggest that under-triage is related to inadequate symptom description. We recommend that caller and call-handler collaborate systematically on problem identification and negotiate non-normative symptom description.
电话咨询和分诊用于限制急诊科的工作量。与面对面咨询相比,电话咨询缺乏视觉线索和临床检查,处于劣势,增加了分诊不足的风险。电话分诊中会出现分诊不足的情况;然而,分诊不足发生的原因尚未得到探讨。本研究的目的是描述实际发生分诊不足的情况,评估分诊不足电话的质量,并确定丹麦首都地区一家区域非工作时间服务机构中导致分诊不足的沟通模式。
选择采用主题分析和描述性统计的解释性同步混合方法。该研究在丹麦哥本哈根首都地区的一家非工作时间服务机构(OOH)中进行。根据特定标准,将分诊不足定义为非工作时间热线的潜在分诊不足电话(PUTC),并通过整合三个数据库进行识别:医疗热线数据库、紧急号码数据库(包括救护车数据库)和电子病历。使用国际疾病分类第十版(ICD - 10)编码对PUTC进行分类,以识别诊断结果,并通过对分诊不足的录音电话进行定性分析确定主要主题。研究期间为2014年10月15日至11月30日。
共识别出327个PUTC,占所有打给OOH电话(n = 937,056)的0.04%。根据诊断结果,PUTC的分布情况为:消化系统(24%)、循环系统(19%)、呼吸系统(15%)和其他所有系统(42%)。对语音记录的主题分析表明,沟通不足和症状描述不规范导致了分诊不足。
潜在分诊不足的发生率较低(0.04%)。然而,消化系统、循环系统和呼吸系统诊断结果的占比过高可能表明分诊不足与症状描述不充分有关。我们建议来电者和接听者在问题识别方面进行系统协作,并就不规范的症状描述进行协商。
分诊不足的发生率较低(0.04%)。然而,消化系统、循环系统和呼吸系统诊断结果的占比过高可能表明分诊不足与症状描述不充分有关。我们建议来电者和接听者在问题识别方面进行系统协作,并就不规范的症状描述进行协商。