Renal and Vascular Inflammation Section, Department of Medicine, Imperial College London, London, UK.
Renal and Vascular Inflammation Section, Department of Medicine, Imperial College London, London, UK.
Kidney Int. 2017 Sep;92(3):693-702. doi: 10.1016/j.kint.2017.03.014. Epub 2017 May 12.
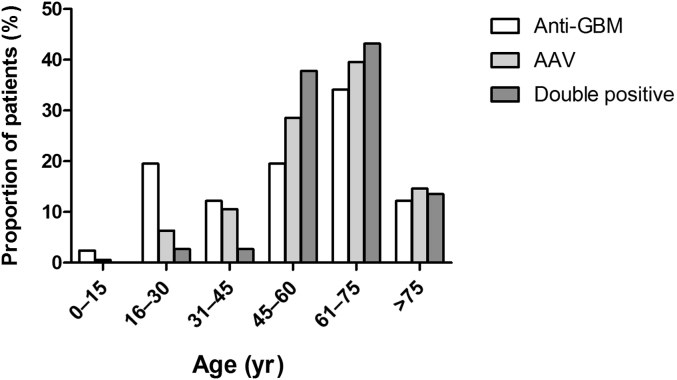
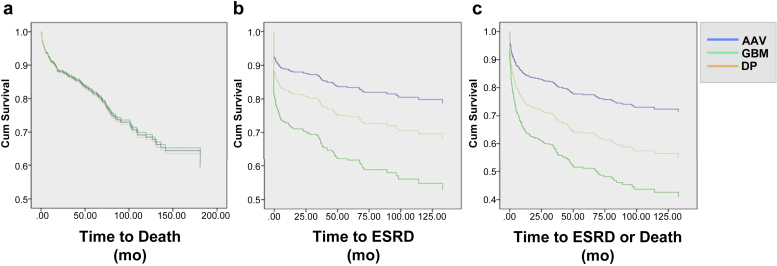
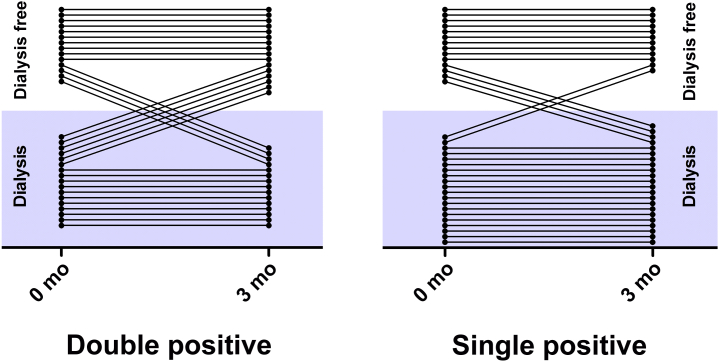
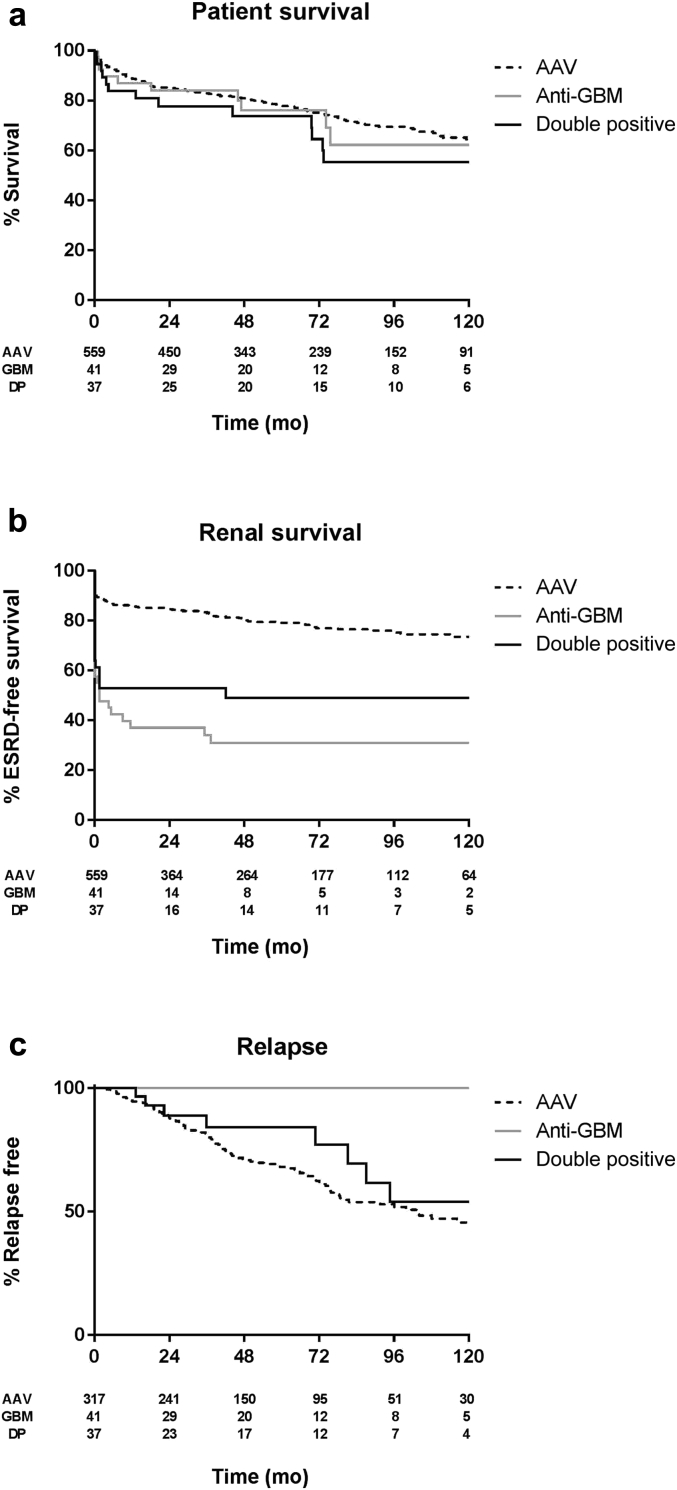
Co-presentation with both ANCA and anti-GBM antibodies is thought to be relatively rare. Current studies of such 'double-positive' cases report small numbers and variable outcomes. To study this further we retrospectively analyzed clinical features and long-term outcomes of a large cohort of 568 contemporary patients with ANCA-associated vasculitis, 41 patients with anti-GBM disease, and 37 double-positive patients with ANCA and anti-GBM disease from four European centers. Double-positive patients shared characteristics of ANCA-associated vasculitis (AAV), such as older age distribution and longer symptom duration before diagnosis, and features of anti-GBM disease, such as severe renal disease and high frequency of lung hemorrhage at presentation. Despite having more evidence of chronic injury on renal biopsy compared to patients with anti-GBM disease, double-positive patients had a greater tendency to recover from being dialysis-dependent after treatment and had intermediate long-term renal survival compared to the single-positive patients. However, overall patient survival was similar in all three groups. Predictors of poor patient survival included advanced age, severe renal failure, and lung hemorrhage at presentation. No single-positive anti-GBM patients experienced disease relapse, whereas approximately half of surviving patients with AAV and double-positive patients had recurrent disease during a median follow-up of 4.8 years. Thus, double-positive patients have a truly hybrid disease phenotype, requiring aggressive early treatment for anti-GBM disease, and careful long-term follow-up and consideration for maintenance immunosuppression for AAV. Since double-positivity appears common, further work is required to define the underlying mechanisms of this association and define optimum treatment strategies.
同时存在抗中性粒细胞胞质抗体 (ANCA) 和抗肾小球基底膜 (GBM) 抗体被认为相对罕见。目前对这类“双阳性”病例的研究报告数量较少且结果不一。为了进一步研究这一问题,我们回顾性分析了来自四个欧洲中心的 568 例当代抗中性粒细胞胞质抗体相关性血管炎患者、41 例抗 GBM 病患者和 37 例抗中性粒细胞胞质抗体和抗 GBM 病双阳性患者的临床特征和长期结局。双阳性患者具有抗中性粒细胞胞质抗体相关性血管炎(AAV)的特征,如年龄分布较老,诊断前症状持续时间较长,以及抗 GBM 病的特征,如严重的肾脏疾病和高频率的肺出血。尽管与抗 GBM 病患者相比,双阳性患者的肾活检更有慢性损伤的证据,但与单阳性患者相比,双阳性患者在治疗后从透析依赖中恢复的趋势更大,且具有中间的长期肾脏存活率。然而,所有三组患者的总体生存率相似。患者生存率差的预测因素包括年龄较大、严重肾功能衰竭和肺出血。没有单阳性抗 GBM 患者出现疾病复发,而大约一半的存活 AAV 患者和双阳性患者在中位随访 4.8 年后出现疾病复发。因此,双阳性患者具有真正的混合疾病表型,需要积极早期治疗抗 GBM 病,并仔细长期随访和考虑维持免疫抑制治疗 AAV。由于双阳性似乎很常见,需要进一步研究以确定这种关联的潜在机制并定义最佳治疗策略。