Brunner Hermine I, Ruperto Nicolino, Tzaribachev Nikolay, Horneff Gerd, Chasnyk Vyacheslav G, Panaviene Violeta, Abud-Mendoza Carlos, Reiff Andreas, Alexeeva Ekaterina, Rubio-Pérez Nadina, Keltsev Vladimir, Kingsbury Daniel J, Del Rocio Maldonado Velázquez Maria, Nikishina Irina, Silverman Earl D, Joos Rik, Smolewska Elzbieta, Bandeira Márcia, Minden Kirsten, van Royen-Kerkhof Annet, Emminger Wolfgang, Foeldvari Ivan, Lauwerys Bernard R, Sztajnbok Flavio, Gilmer Keith E, Xu Zhenhua, Leu Jocelyn H, Kim Lilianne, Lamberth Sarah L, Loza Matthew J, Lovell Daniel J, Martini Alberto
Cincinnati Children's Hospital Medical Center, Cincinnati, Ohio, USA.
Istituto Giannina Gaslini, Pediatria II - Rheumatologia, PRINTO, Genoa, Italy.
Ann Rheum Dis. 2018 Jan;77(1):21-29. doi: 10.1136/annrheumdis-2016-210456. Epub 2017 May 15.
This report aims to determine the safety, pharmacokinetics (PK) and efficacy of subcutaneous golimumab in active polyarticular-course juvenile idiopathic arthritis (polyJIA).
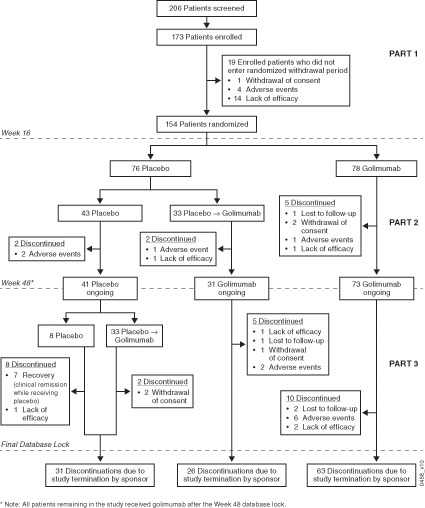
In this three-part randomised double-blinded placebo-controlled withdrawal trial, all patients received open-label golimumab (30 mg/m of body surface area; maximum: 50 mg/dose) every 4 weeks together with weekly methotrexate during Part 1 (weeks 0-16). Patients with at least 30% improvement per American College of Rheumatology Criteria for JIA (JIA ACR30) in Part 1 entered the double-blinded Part 2 (weeks 16-48) after 1:1 randomisation to continue golimumab or start placebo. In Part 3, golimumab was continued or could be restarted as in Part 1. The primary outcome was JIA flares in Part 2; secondary outcomes included JIA ACR50/70/90 responses, clinical remission, PK and safety.
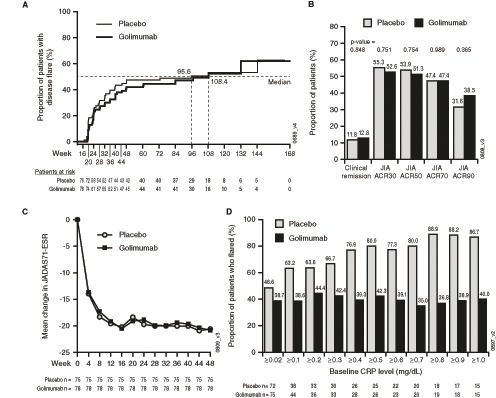
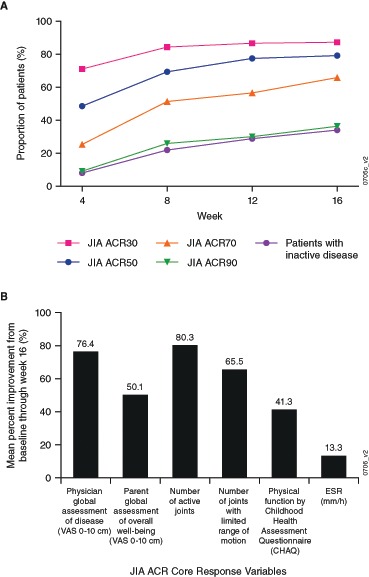
Among 173 patients with polyJIA enrolled, 89.0% (154/173) had a JIA ACR30 response and 79.2%/65.9%/36.4% demonstrated JIA ACR50/70/90 responses in Part 1. At week 48, the primary endpoint was not met as treatment groups had comparable JIA flare rates (golimumab vs placebo: 32/78=41% vs 36/76=47%; p=0.41), and rates of clinical remission were comparable (golimumab vs placebo: 10/78=12.8% vs 9/76=11.8%). Adverse event and serious adverse event rates were similar in the treatment groups during Part 2. Injection site reactions occurred with <1% of all injections. PK analysis confirmed adequate golimumab dosing for polyJIA.
Although the primary endpoint was not met, golimumab resulted in rapid, clinically meaningful, improvement in children with active polyJIA. Golimumab was well tolerated, and no unexpected safety events occurred.
NCT01230827; Results.
本报告旨在确定皮下注射戈利木单抗治疗活动期多关节型幼年特发性关节炎(polyJIA)的安全性、药代动力学(PK)和疗效。
在这项三部分的随机双盲安慰剂对照撤药试验中,在第1部分(0-16周),所有患者每4周接受一次开放标签的戈利木单抗(30mg/m²体表面积;最大剂量:50mg/剂),同时每周服用甲氨蝶呤。在第1部分中,根据美国风湿病学会幼年特发性关节炎标准(JIA ACR30)改善至少30%的患者在1:1随机分组后进入双盲第2部分(16-48周),继续使用戈利木单抗或开始使用安慰剂。在第3部分,戈利木单抗按第1部分的方案继续使用或可重新开始使用。主要结局是第2部分中的JIA病情复发;次要结局包括JIA ACR50/70/90反应、临床缓解、PK和安全性。
在纳入的173例polyJIA患者中,89.0%(154/173)有JIA ACR30反应,79.2%/65.9%/36.4%在第1部分表现出JIA ACR50/70/90反应。在第48周时,未达到主要终点,因为治疗组的JIA病情复发率相当(戈利木单抗组与安慰剂组:32/78 = 41% 对 36/76 = 47%;p = 0.41),临床缓解率也相当(戈利木单抗组与安慰剂组:10/78 = 12.8% 对 9/76 = 11.8%)。在第2部分中,治疗组的不良事件和严重不良事件发生率相似。所有注射中<1%发生注射部位反应PK分析证实戈利木单抗对polyJIA的给药剂量合适。
虽然未达到主要终点,但戈利木单抗使活动期polyJIA患儿迅速获得了具有临床意义的改善。戈利木单抗耐受性良好,未发生意外的安全事件。
NCT01230827;结果。