Zhang Ling, Wu Hai-Wei, Yuan Weien, Zheng Jia-Wei
Department of Oral-Maxillary Head and Neck, Ninth People's Hospital, College of Stomatology, Shanghai Jiao Tong University School of Medicine, Shanghai Key Laboratory of Stomatology, Shanghai.
School of Pharmacy, Shanghai Jiao Tong University, Shanghai, People's Republic of China.
Drug Des Devel Ther. 2017 May 8;11:1401-1408. doi: 10.2147/DDDT.S134808. eCollection 2017.
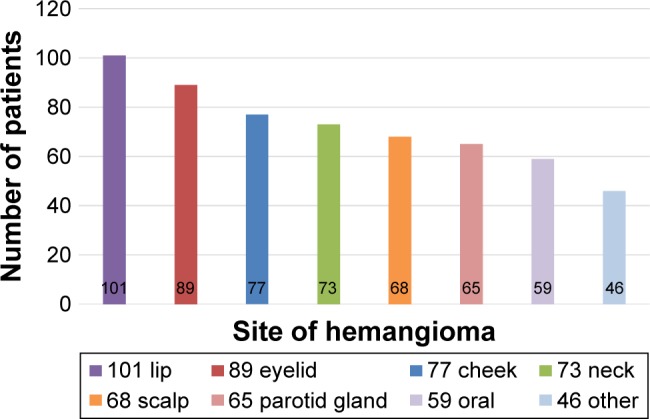
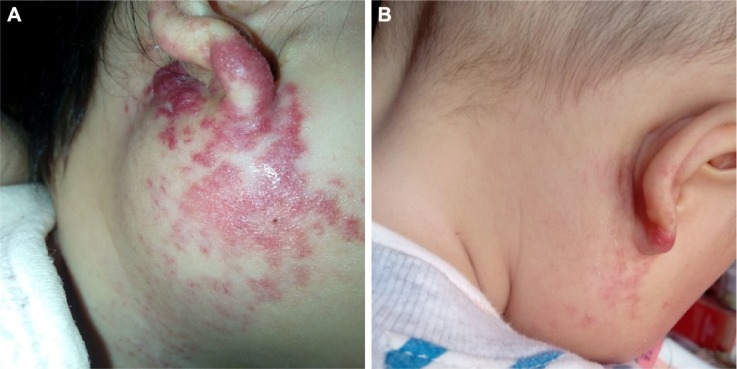
Hemangiomas are the most common benign vascular tumors of infancy. Although most infantile hemangiomas (IHs) have the ability to involute spontaneously after initial proliferation and resolve without consequence, intervention is required in a subset of IHs, which develop complications resulting in ulceration, bleeding, or aesthetic deformity. The primary treatment for this subset of IHs is pharmacological intervention, and propranolol has become the new first-line treatment for complicated hemangiomas. Here, we evaluated the efficacy of propranolol on proliferation IH in a clinical cohort including 578 patients.
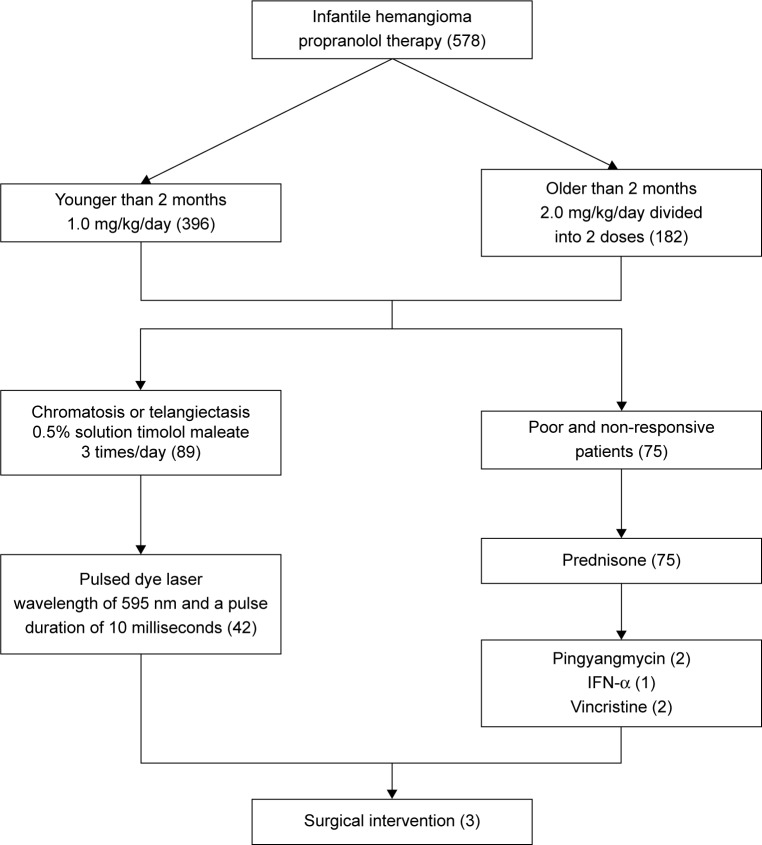
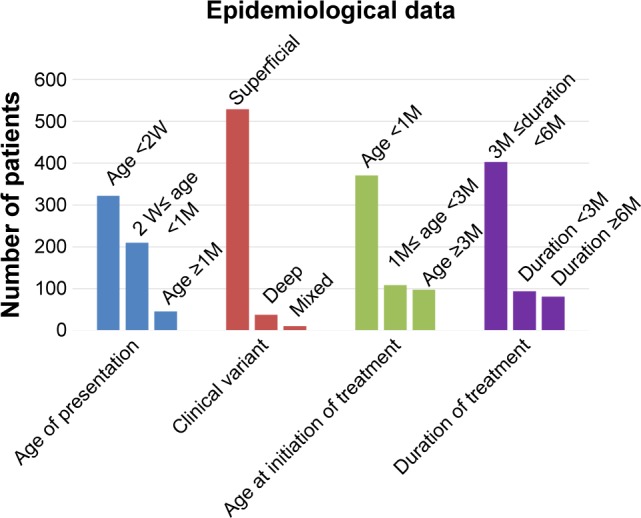
We retrospectively reviewed a total of 578 IH patients who were treated with oral propranolol from January 2010 to December 2012. Responses to the propranolol treatment were graded as: excellent, good, poor, or no response. Based on the response to propranolol treatment (once daily at a dose of 1.0 mg/kg for patients younger than 2 months; twice daily at daily total dose of 2 mg/kg for patients older than 2 months), additional pharmacotherapies or surgery were used for IH patients for satisfactory clinical outcome.
Five hundred and sixty (96.9%) of 578 IH patients in our study responded to oral propranolol treatment, and the response rate was significantly different for different ages of patients (<0.05), with the youngest patients having the highest response rate. The mean time of treatment was 6 months (range, 3-12 months). For example, response rate to propranolol was 98.1% in patients younger than 2 months, compared with 93.3% in patients older than 2 months and younger than 8 months, and 73.7% in patients older than 8 months. One hundred and thirty one patients who exhibited incompletely involuted hemangiomas were further treated with timolol maleate (n=89) or pulsed dye laser (n=42). One hundred and seventeen (89.3%) of 131 patients showed a positive response. There were no instances of life-threatening complications after propranolol. However, minor side effects were observed including 10 (1.73%) cases of sleep disturbance, 7 (1.21%) cases of diarrhea, and 5 (0.86%) cases of bronchospasm.
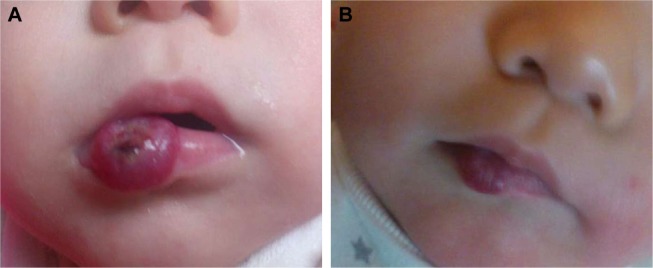
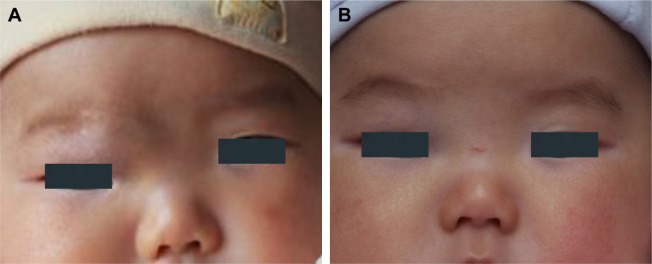
IH requires early intervention. During the involution phase, tapering propranolol dosage can be done to minimize side effects before discontinuing treatment. For patients exhibiting telangiectasia and chromatosis after propranolol treatment, administration of a 0.5% solution of timolol maleate or pulse dye laser is an effective therapeutic approach for complete involution.
血管瘤是婴儿期最常见的良性血管肿瘤。虽然大多数婴儿血管瘤(IHs)在初始增殖后有自行消退的能力且消退后无不良后果,但一部分IHs需要干预,因为它们会出现导致溃疡、出血或美观畸形的并发症。这部分IHs的主要治疗方法是药物干预,普萘洛尔已成为治疗复杂血管瘤的新一线治疗药物。在此,我们评估了普萘洛尔在一个包括578例患者的临床队列中对增殖期IH的疗效。
我们回顾性分析了2010年1月至2012年12月期间接受口服普萘洛尔治疗的578例IH患者。对普萘洛尔治疗的反应分为:优、良、差或无反应。根据对普萘洛尔治疗的反应(2个月以下患者每日一次,剂量为1.0mg/kg;2个月以上患者每日两次,每日总剂量为2mg/kg),对IH患者采用额外的药物治疗或手术以获得满意的临床结果。
我们研究中的578例IH患者中有560例(96.9%)对口服普萘洛尔治疗有反应,不同年龄患者的反应率有显著差异(<0.05),年龄最小的患者反应率最高。平均治疗时间为6个月(范围3 - 12个月)。例如,2个月以下患者对普萘洛尔的反应率为98.1%,2个月以上且8个月以下患者为93.3%,8个月以上患者为73.7%。131例血管瘤未完全消退的患者进一步接受了马来酸噻吗洛尔治疗(n = 89)或脉冲染料激光治疗(n = 42)。131例患者中有117例(89.3%)显示出阳性反应。普萘洛尔治疗后未出现危及生命的并发症。然而,观察到了一些轻微的副作用,包括10例(1.73%)睡眠障碍、7例(1.21%)腹泻和5例(0.86%)支气管痉挛。
IH需要早期干预。在消退期,可以逐渐减少普萘洛尔剂量以在停药前将副作用降至最低。对于普萘洛尔治疗后出现毛细血管扩张和色素沉着的患者,给予0.5%的马来酸噻吗洛尔溶液或脉冲染料激光治疗是实现完全消退的有效治疗方法。