Kose Kamil Cagri, Bozduman Omer, Yenigul Ali Erkan, Igrek Servet
Marmara University Faculty of Medicine Department of Orthopedics and Traumatology, Istanbul, Turkey.
Ufuk University Faculty of Medicine Department of Orthopaedics and Traumatology, Ankara, Turkey.
EFORT Open Rev. 2017 Apr 27;2(3):73-82. doi: 10.1302/2058-5241.2.160069. eCollection 2017 Mar.
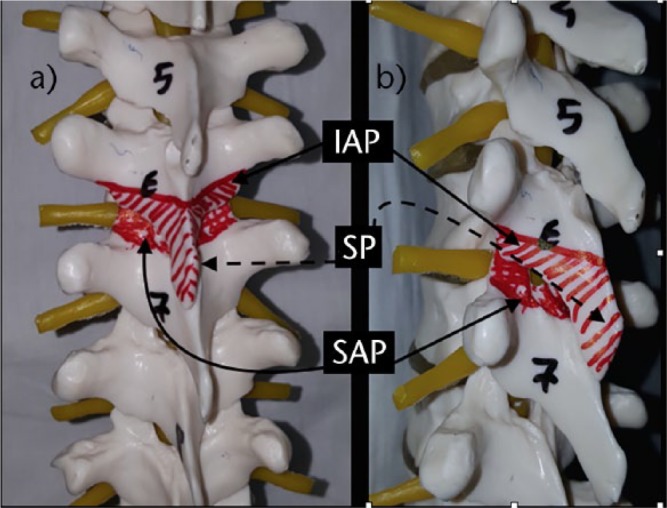
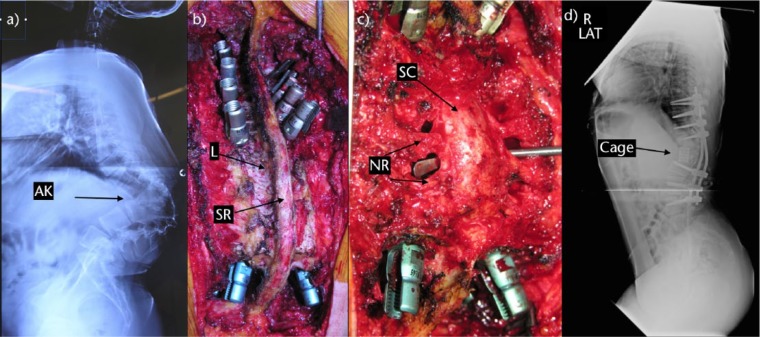
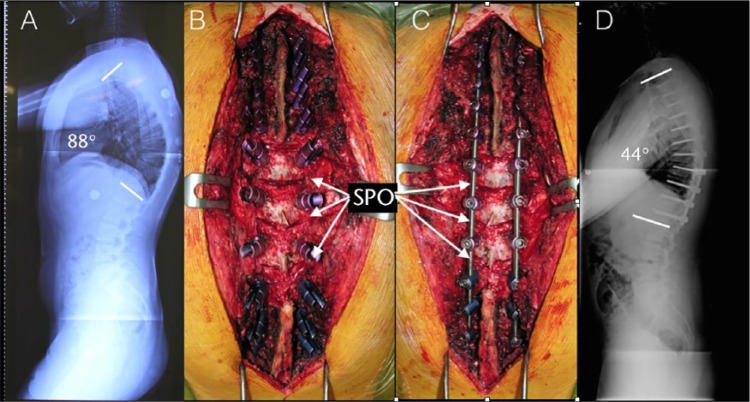
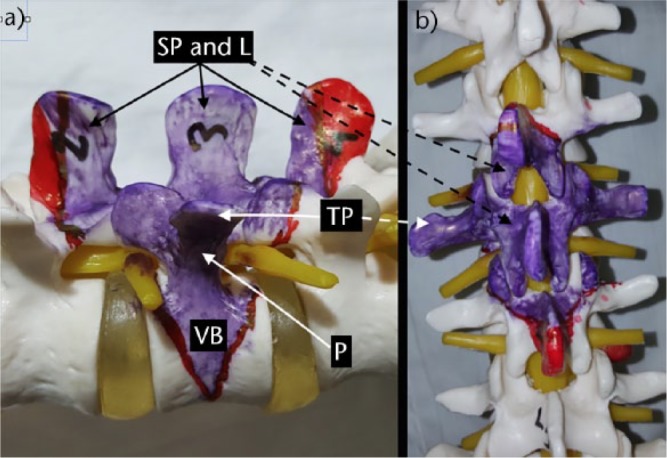
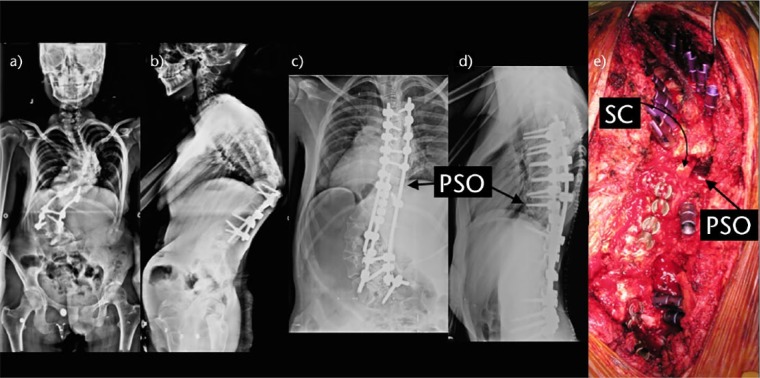
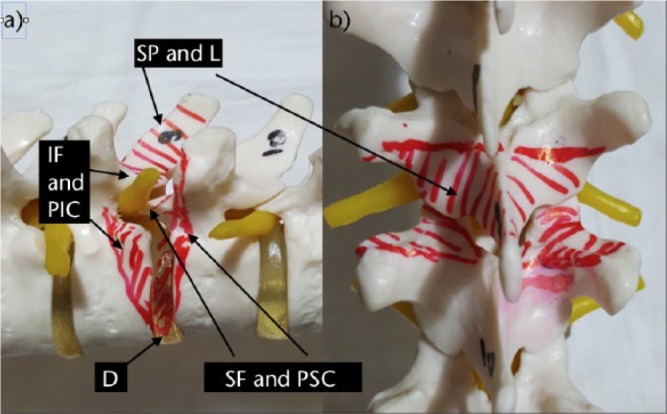
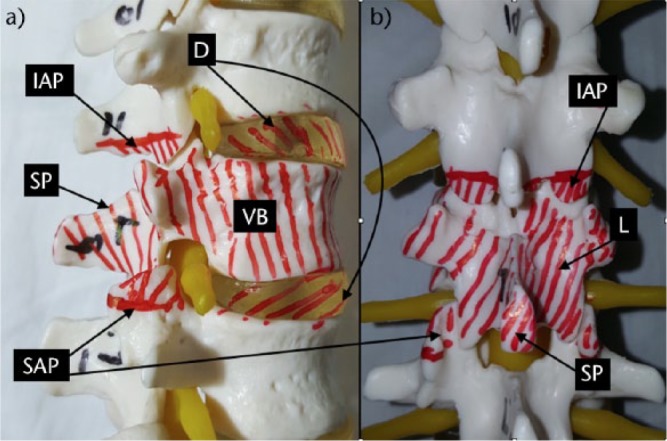
The aims of spinal deformity surgery are to achieve balance, relieve pain and prevent recurrence or worsening of the deformity.The main types of osteotomies are the Smith-Petersen osteotomy (SPO), pedicle subtraction osteotomy (PSO), bone-disc-bone osteotomy (BDBO) and vertebral column resection (VCR), in order of increasing complexity.SPO is a posterior column osteotomy in which the posterior ligaments and the facet joints are removed and correction is performed through the disc space. A mobile anterior disc is essential. SPO is best in patients with +6-8 cm C7 plumbline. The amount of correction is 9.3° to 10.7°/level (1°/mm bone).PSO is a technique where the posterior elements and pedicles are removed. Then a triangular wedge through the pedicles is removed and the posterior spine is shortened using the anterior cortex as a hinge. The ideal candidates are patients with a severe sagittal imbalance. A single level osteotomy can produce 30° 40° of correction. A single level osteotomy may restore global sagittal balance by an average of 9 cm with an upper limit of 19 cm.BDBO is an osteotomy done above and below a disc level. A BDBO provides correction rates in the range of 35° to 60°. The main indications are deformities with the disc space as the apex and severe sagittal plane deformities.VCR is indicated for rigid multi-planar deformities, sharp angulated deformities, hemivertebra resections, resectable spinal tumours, post-traumatic deformities and spondyloptosis. The main indication for a VCR is fixed coronal plane deformity.The type of osteotomy must be chosen mainly according to the aetiology, type and apex of the deformity. One may start with SPOs and may gradually advance to complex osteotomies. Cite this article: 2017;2:73-82. DOI: 10.1302/2058-5241.2.160069.
脊柱畸形手术的目的是实现平衡、缓解疼痛并防止畸形复发或加重。截骨术的主要类型依次为史密斯-彼得森截骨术(SPO)、经椎弓根截骨术(PSO)、骨-椎间盘-骨截骨术(BDBO)和脊柱全椎体切除术(VCR),其复杂程度逐渐增加。SPO是一种后柱截骨术,术中需切除后韧带和小关节,并通过椎间盘间隙进行矫正。一个可活动的前方椎间盘至关重要。SPO最适合C7铅垂线偏移量为+6 - 8 cm的患者。矫正量为9.3°至10.7°/节段(1°/mm骨质)。PSO是一种切除后方结构和椎弓根的技术。然后通过椎弓根切除一个三角形骨块,并以前侧皮质为铰链缩短后脊柱。理想的手术对象是矢状面严重失衡的患者。单节段截骨可产生30°至40°的矫正。单节段截骨平均可恢复整体矢状面平衡9 cm,上限为19 cm。BDBO是在椎间盘上下进行的截骨术。BDBO的矫正率在35°至60°之间。主要适应证是以椎间盘间隙为顶点的畸形和严重矢状面畸形。VCR适用于僵硬的多平面畸形、锐角畸形、半椎体切除、可切除的脊柱肿瘤、创伤后畸形和椎体滑脱。VCR的主要适应证是固定的冠状面畸形。截骨术的类型必须主要根据畸形的病因、类型和顶点来选择。可以从SPO开始,逐渐过渡到复杂的截骨术。引用本文:2017;2:73 - 82。DOI:10.1302/2058 - 5241.2.160069。