Tsugawa Yusuke, Newhouse Joseph P, Zaslavsky Alan M, Blumenthal Daniel M, Jena Anupam B
Department of Health Policy and Management, Harvard T. H. Chan School of Public Health, Boston, MA, USA
Division of General Internal Medicine and Primary Care, Brigham and Women's Hospital, Boston, MA, USA.
BMJ. 2017 May 16;357:j1797. doi: 10.1136/bmj.j1797.
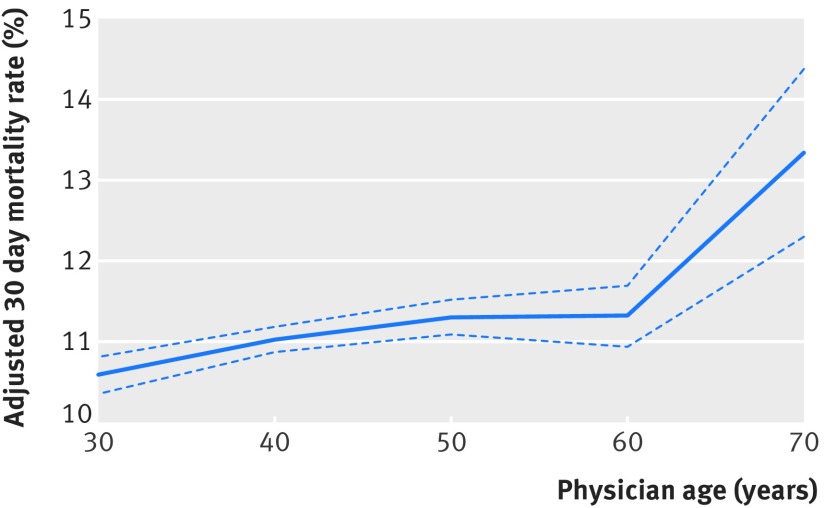
To investigate whether outcomes of patients who were admitted to hospital differ between those treated by younger and older physicians. Observational study. US acute care hospitals. 20% random sample of Medicare fee-for-service beneficiaries aged ≥65 admitted to hospital with a medical condition in 2011-14 and treated by hospitalist physicians to whom they were assigned based on scheduled work shifts. To assess the generalizability of findings, analyses also included patients treated by general internists including both hospitalists and non-hospitalists. 30 day mortality and readmissions and costs of care. 736 537 admissions managed by 18 854 hospitalist physicians (median age 41) were included. Patients' characteristics were similar across physician ages. After adjustment for characteristics of patients and physicians and hospital fixed effects (effectively comparing physicians within the same hospital), patients' adjusted 30 day mortality rates were 10.8% for physicians aged <40 (95% confidence interval 10.7% to 10.9%), 11.1% for physicians aged 40-49 (11.0% to 11.3%), 11.3% for physicians aged 50-59 (11.1% to 11.5%), and 12.1% for physicians aged ≥60 (11.6% to 12.5%). Among physicians with a high volume of patients, however, there was no association between physician age and patient mortality. Readmissions did not vary with physician age, while costs of care were slightly higher among older physicians. Similar patterns were observed among general internists and in several sensitivity analyses. Within the same hospital, patients treated by older physicians had higher mortality than patients cared for by younger physicians, except those physicians treating high volumes of patients.
调查入住医院的患者在年轻医生和年长医生治疗下的结局是否存在差异。观察性研究。美国急症护理医院。2011 - 2014年期间,从年龄≥65岁因医疗状况入住医院并由根据排班工作班次分配给他们的住院医师治疗的医疗保险按服务收费受益人中随机抽取20%的样本。为评估研究结果的普遍性,分析还纳入了由普通内科医生(包括住院医师和非住院医师)治疗的患者。30天死亡率、再入院率和护理费用。纳入了由18854名住院医师(中位年龄41岁)管理的736537例入院病例。不同年龄医生治疗的患者特征相似。在对患者和医生的特征以及医院固定效应进行调整后(实际上是在同一医院内比较医生),年龄<40岁的医生治疗的患者调整后30天死亡率为10.8%(95%置信区间10.7%至10.9%),40 - 49岁的医生为11.1%(11.0%至11.3%),50 - 59岁的医生为11.3%(11.1%至11.5%),≥60岁的医生为12.1%(11.6%至12.5%)。然而,在患者量大的医生中,医生年龄与患者死亡率之间没有关联。再入院率与医生年龄无关,而年长医生的护理费用略高。在普通内科医生中以及在几项敏感性分析中也观察到了类似模式。在同一医院内,除了那些治疗大量患者的医生外,年长医生治疗的患者死亡率高于年轻医生治疗的患者。