Luckenbaugh Amy N, Marks Rory M, Miller David C, Weizer Alon Z, Stoffel John T, Montgomery Jeffrey S
Department of Urology, University of Michigan Health System, Ann Arbor, MI, USA.
Department of Internal Medicine, University of Michigan Health System, Ann Arbor, MI, USA.
Bladder Cancer. 2017 Apr 27;3(2):133-138. doi: 10.3233/BLC-160089.
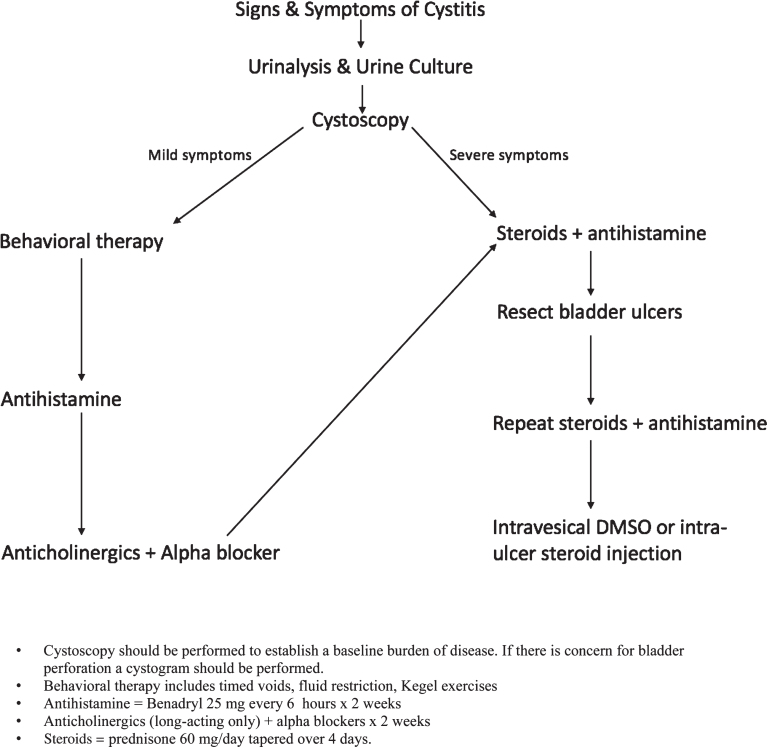
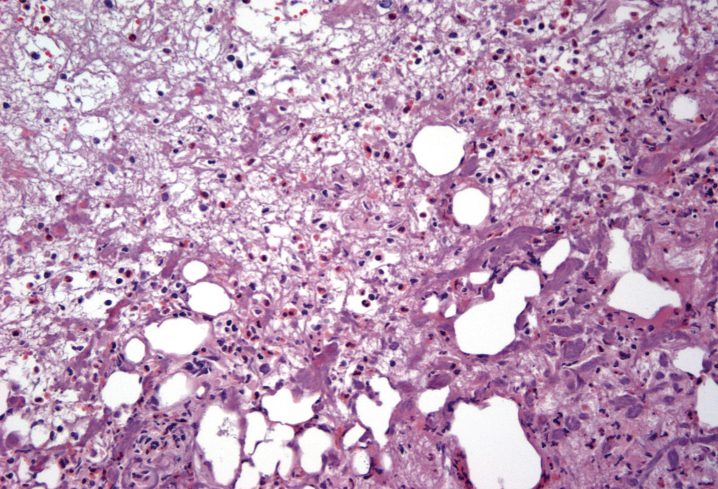
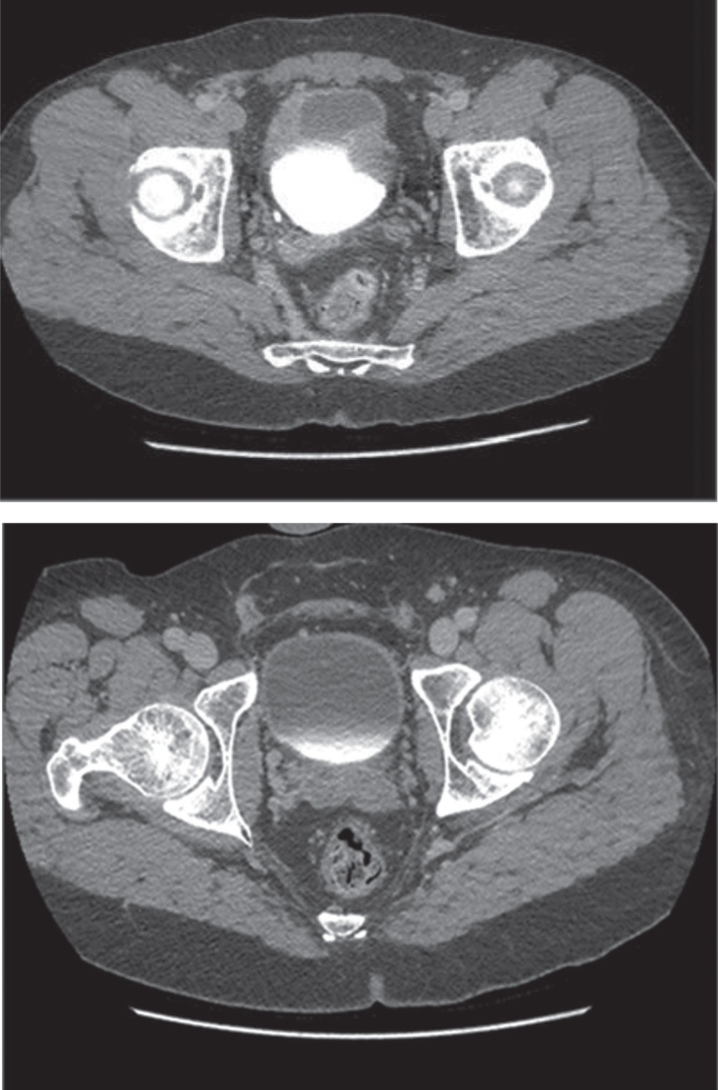
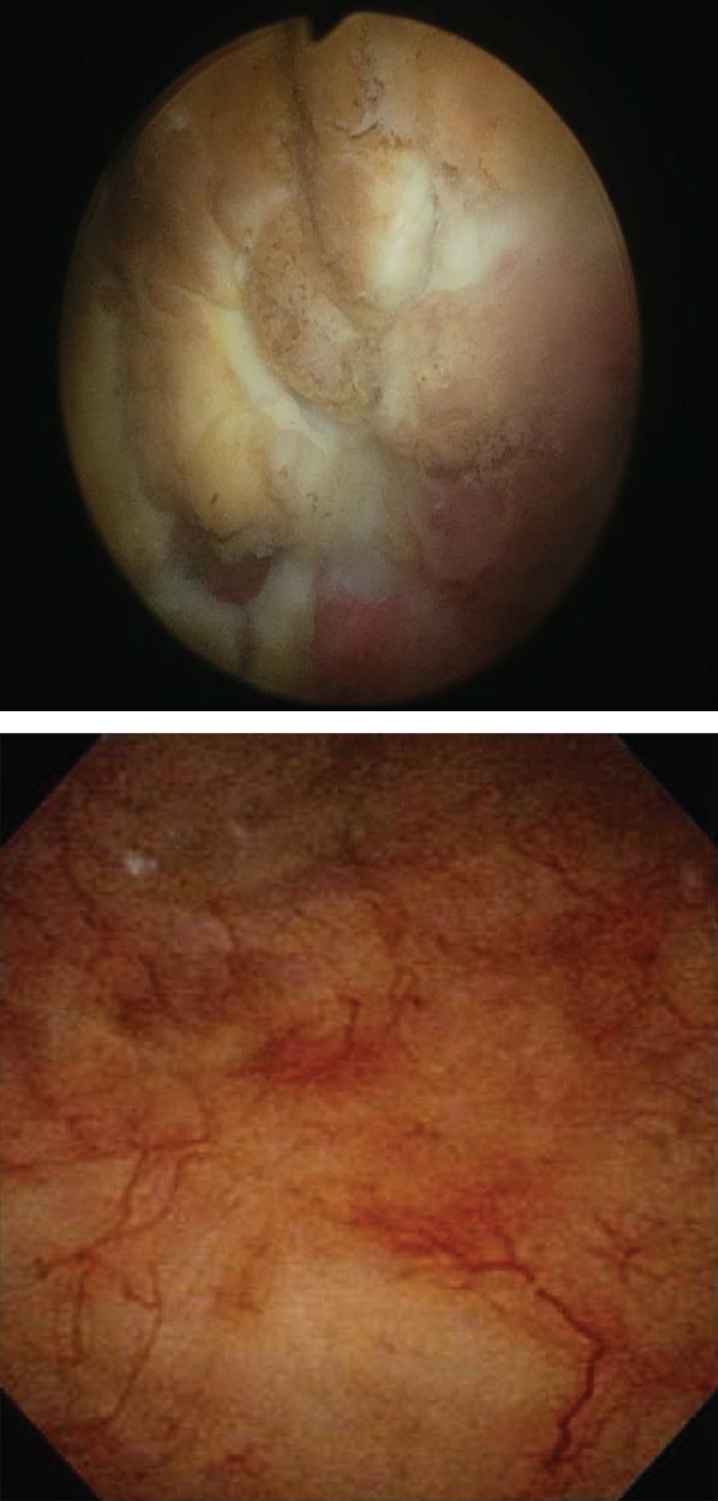
A post-bladder tumor resection dose of MMC can reduce non-invasive papillary (pTa) bladder cancer recurrences by up to 40%; this treatment is recommended in both the AUA and EUA non-muscle-invasive bladder cancer guidelines. A common complication of this treatment is eosinophilic cystitis. Symptoms range from mild urinary frequency and urgency to debilitating pain and dysuria. Currently, there is no established treatment algorithm for MMC-induced cystitis. Members of the Urologic Surgery Quality Collaborative (USQC), a group composed of over 160 private and academic urologists, met to discuss the management of patients with cystitis following MMC therapy. They devised a treatment algorithm based on experiences of urologic oncologists and neurourologists to aid in the diagnosis and management of MMC-induced cystitis. The assessment begins with urinalysis and culture, followed by cystoscopy. For mild symptoms, behavioral therapy, including timed voids, fluid restriction and Kegel exercises are trialed. If symptoms have not resolved, treatment with an antihistamine, followed by a combination of anticholinergic and alpha-blocker medications. For persistent symptoms or severe symptoms at presentation, a course of prednisone plus antihistamine is prescribed. If symptoms are improving but have not resolved, this treatment is extended for a full 4 weeks prior to steroid taper. If symptoms do not improve, any visible bladder ulcerations are resected intraoperatively followed by an additional course of prednisone and antihistamine. Intravesical DMSO instillations and intra-ulcer steroid injection can be used as a final effort to treat this condition. We present the first formal management algorithm with escalating treatment intensity tailored to patient symptoms.
膀胱肿瘤切除术后使用丝裂霉素(MMC)的剂量可将非侵袭性乳头状(pTa)膀胱癌的复发率降低多达40%;美国泌尿外科学会(AUA)和欧洲泌尿外科学会(EUA)的非肌层浸润性膀胱癌指南均推荐这种治疗方法。这种治疗的常见并发症是嗜酸性膀胱炎。症状从轻微的尿频和尿急到使人虚弱的疼痛及排尿困难不等。目前,对于MMC诱发的膀胱炎尚无既定的治疗方案。由160多名私立和学术性泌尿科医生组成的泌尿外科手术质量协作组(USQC)成员开会讨论了MMC治疗后膀胱炎患者的管理。他们根据泌尿肿瘤学家和神经泌尿科医生的经验设计了一种治疗方案,以协助诊断和管理MMC诱发的膀胱炎。评估从尿液分析和培养开始,随后进行膀胱镜检查。对于轻度症状,尝试行为疗法,包括定时排尿、限制液体摄入和凯格尔运动。如果症状没有缓解,则使用抗组胺药治疗,随后联合使用抗胆碱能药物和α受体阻滞剂。对于持续症状或就诊时的严重症状,开具泼尼松加抗组胺药的疗程。如果症状正在改善但尚未缓解,则在逐渐减少类固醇剂量之前将这种治疗延长整整4周。如果症状没有改善,则在术中切除任何可见的膀胱溃疡,随后再进行一个疗程的泼尼松和抗组胺药治疗。膀胱内灌注二甲基亚砜(DMSO)和溃疡内注射类固醇可作为治疗这种疾病的最后手段。我们提出了首个根据患者症状调整治疗强度的正式管理方案。