Träger Karl, Skrabal Christian, Fischer Guenther, Datzmann Thomas, Schroeder Janpeter, Fritzler Daniel, Hartmann Jan, Liebold Andreas, Reinelt Helmut
Department of Cardiac Anesthesiology, University Hospital Ulm, Ulm - Germany.
Clinic of Cardiothoracic and Vascular Surgery, University Hospital Ulm, Ulm - Germany.
Int J Artif Organs. 2017 May 29;40(5):240-249. doi: 10.5301/ijao.5000583. Epub 2017 May 19.
Infective endocarditis is a serious disease condition. Depending on the causative microorganism and clinical symptoms, cardiac surgery and valve replacement may be needed, posing additional risks to patients who may simultaneously suffer from septic shock. The combination of surgery bacterial spreadout and artificial cardiopulmonary bypass (CPB) surfaces results in a release of key inflammatory mediators leading to an overshooting systemic hyperinflammatory state frequently associated with compromised hemodynamic and organ function. Hemoadsorption might represent a potential approach to control the hyperinflammatory systemic reaction associated with the procedure itself and subsequent clinical conditions by reducing a broad range of immuno-regulatory mediators.
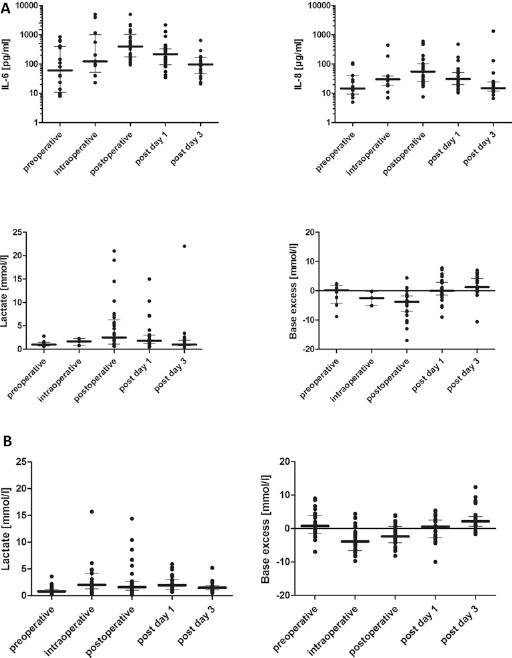
We describe 39 cardiac surgery patients with proven acute infective endocarditis obtaining valve replacement during CPB surgery in combination with intraoperative CytoSorb hemoadsorption. In comparison, we evaluated a historical group of 28 patients with infective endocarditis undergoing CPB surgery without intraoperative hemoadsorption.
CytoSorb treatment was associated with a mitigated postoperative response of key cytokines and clinical metabolic parameters. Moreover, patients showed hemodynamic stability during and after the operation while the need for vasopressors was less pronounced within hours after completion of the procedure, which possibly could be attributed to the additional CytoSorb treatment. Intraoperative hemoperfusion treatment was well tolerated and safe without the occurrence of any CytoSorb device-related adverse event.
Thus, this interventional approach may open up potentially promising therapeutic options for critically-ill patients with acute infective endocarditis during and after cardiac surgery, with cytokine reduction, improved hemodynamic stability and organ function as seen in our patients.
感染性心内膜炎是一种严重的疾病状态。根据致病微生物和临床症状,可能需要进行心脏手术和瓣膜置换,这给可能同时患有感染性休克的患者带来了额外风险。手术中细菌的扩散和人工心肺转流(CPB)表面导致关键炎症介质的释放,从而引发全身性过度炎症反应,这种反应常与血流动力学和器官功能受损相关。血液吸附可能是一种潜在的方法,通过减少多种免疫调节介质来控制与手术本身及后续临床状况相关的全身性过度炎症反应。
我们描述了39例经证实患有急性感染性心内膜炎的心脏手术患者,他们在CPB手术期间进行瓣膜置换,并在术中联合使用CytoSorb血液吸附。相比之下,我们评估了一组28例历史对照患者,这些患者患有感染性心内膜炎,在CPB手术期间未进行术中血液吸附。
CytoSorb治疗与关键细胞因子和临床代谢参数的术后反应减轻相关。此外,患者在手术期间和术后表现出血流动力学稳定性,并且在手术完成后的数小时内对血管升压药的需求不那么明显,这可能归因于额外的CytoSorb治疗。术中血液灌流治疗耐受性良好且安全,未发生任何与CytoSorb装置相关的不良事件。
因此,这种介入方法可能为心脏手术期间及术后患有急性感染性心内膜炎的重症患者开辟潜在的有前景的治疗选择,如我们的患者所示,可减少细胞因子、改善血流动力学稳定性和器官功能。