Jenks Sara J, Conway Bryan R, McLachlan Stela, Teoh Wei Leng, Williamson Rachel M, Webb David J, Welsh Paul, Sattar Naveed, Strachan Mark W J, Price Jackie F
Department of Clinical Biochemistry, Royal Infirmary of Edinburgh, Edinburgh, UK.
Centre for Population Health Sciences, University of Edinburgh, Old Medical School, Teviot Place, Edinburgh, EH8 9AG, UK.
Diabetologia. 2017 Aug;60(8):1400-1408. doi: 10.1007/s00125-017-4297-0. Epub 2017 May 20.
AIMS/HYPOTHESIS: We investigated whether biochemical cardiovascular risk factors and/or markers of subclinical cardiovascular disease were associated with the development of reduced renal function in people with type 2 diabetes.
A cohort of 1066 Scottish men and women aged 60-74 years with type 2 diabetes from the Edinburgh Type 2 Diabetes Study were followed up for a median of 6.7 years. New-onset reduced renal function was defined as two eGFRs <60 ml min (1.73 m) at least 3 months apart with a > 25% decline from baseline eGFR. Ankle brachial pressure index (ABI), N-terminal pro-B-type natriuretic peptide (NT-proBNP) and high-sensitivity troponin T (hsTnT) were measured at baseline. Pulse wave velocity (PWV) and carotid intima media thickness were measured 1 year into follow-up. Data were analysed using Cox proportional hazards models.
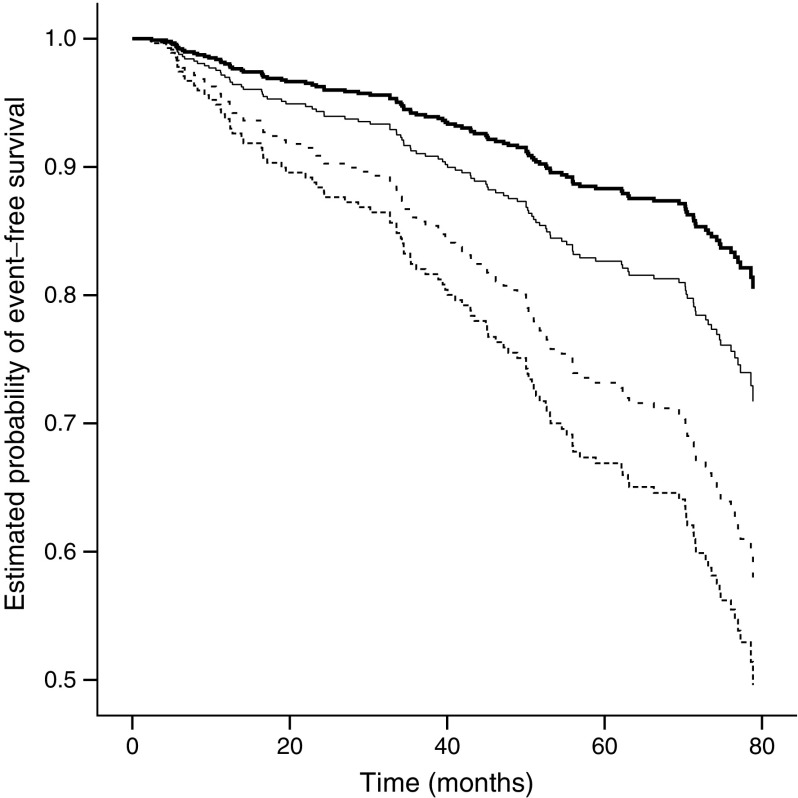
A total of 119 participants developed reduced renal function during follow-up. ABI, PWV, NT-proBNP and hsTnT were all associated with onset of decline in renal function following adjustment for age and sex. These associations were attenuated after adjustment for additional diabetes renal disease risk factors (systolic BP, baseline eGFR, albumin:creatinine ratio and smoking pack-years), with the exception of hsTnT which remained independently associated (HR 1.51 [95% CI 1.22, 1.87]). Inclusion of hsTnT in a predictive model improved the continuous net reclassification index by 0.165 (0.008, 0.286).
CONCLUSIONS/INTERPRETATION: Our findings demonstrate an association between hsTnT, a marker of subclinical cardiac ischaemia, and subsequent renal function decline. Further research is required to establish the predictive value of hsTnT and response to intervention.
目的/假设:我们调查了2型糖尿病患者的生化心血管危险因素和/或亚临床心血管疾病标志物是否与肾功能下降的发生有关。
对1066名来自爱丁堡2型糖尿病研究的60 - 74岁的苏格兰男性和女性进行队列研究,随访时间中位数为6.7年。新发肾功能下降定义为两次估算肾小球滤过率(eGFR)<60 ml/(min·1.73 m²),间隔至少3个月,且较基线eGFR下降>25%。在基线时测量踝臂血压指数(ABI)、N末端B型利钠肽原(NT-proBNP)和高敏肌钙蛋白T(hsTnT)。随访1年时测量脉搏波速度(PWV)和颈动脉内膜中层厚度。使用Cox比例风险模型分析数据。
共有119名参与者在随访期间出现肾功能下降。在调整年龄和性别后,ABI、PWV、NT-proBNP和hsTnT均与肾功能下降的发生有关。在调整了其他糖尿病肾病危险因素(收缩压、基线eGFR、白蛋白与肌酐比值和吸烟包年数)后,这些关联减弱,但hsTnT除外,其仍保持独立关联(风险比1.51 [95%可信区间1.22, 1.87])。将hsTnT纳入预测模型可使连续净重新分类指数提高0.165(0.008, 0.286)。
结论/解读:我们的研究结果表明,亚临床心肌缺血标志物hsTnT与随后的肾功能下降之间存在关联。需要进一步研究以确定hsTnT的预测价值和对干预的反应。