Shah Anoop S V, Griffiths Megan, Lee Kuan Ken, McAllister David A, Hunter Amanda L, Ferry Amy V, Cruikshank Anne, Reid Alan, Stoddart Mary, Strachan Fiona, Walker Simon, Collinson Paul O, Apple Fred S, Gray Alasdair J, Fox Keith A A, Newby David E, Mills Nicholas L
BHF Centre for Cardiovascular Science, University of Edinburgh, Edinburgh EH16 4SB, UK.
Centre for Population Health Sciences, University of Edinburgh, UK.
BMJ. 2015 Jan 21;350:g7873. doi: 10.1136/bmj.g7873.
To evaluate the diagnosis of myocardial infarction using a high sensitivity troponin I assay and sex specific diagnostic thresholds in men and women with suspected acute coronary syndrome.
Prospective cohort study.
Regional cardiac centre, United Kingdom.
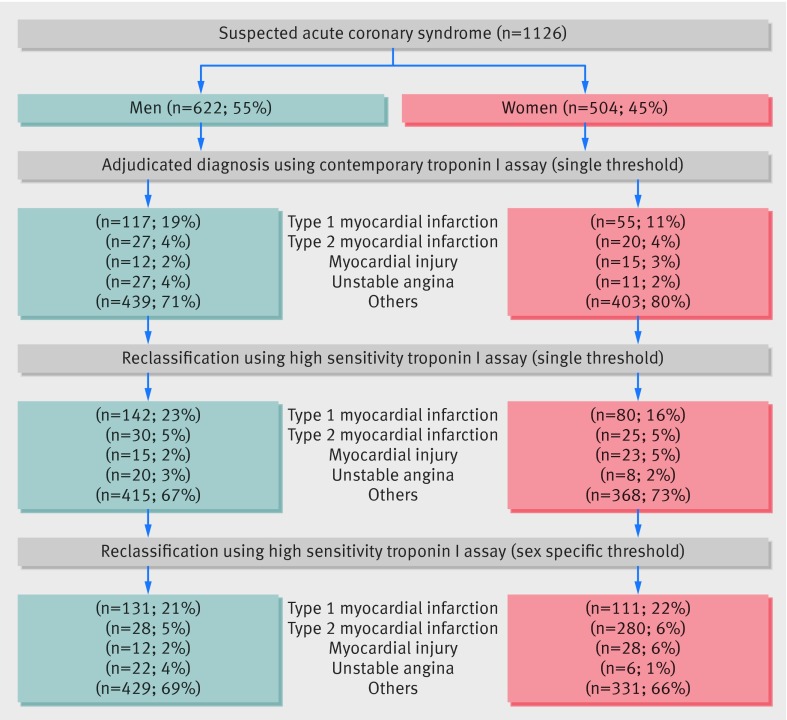
Consecutive patients with suspected acute coronary syndrome (n=1126, 46% women). Two cardiologists independently adjudicated the diagnosis of myocardial infarction by using a high sensitivity troponin I assay with sex specific diagnostic thresholds (men 34 ng/L, women 16 ng/L) and compared with current practice where a contemporary assay (50 ng/L, single threshold) was used to guide care.
Diagnosis of myocardial infarction.
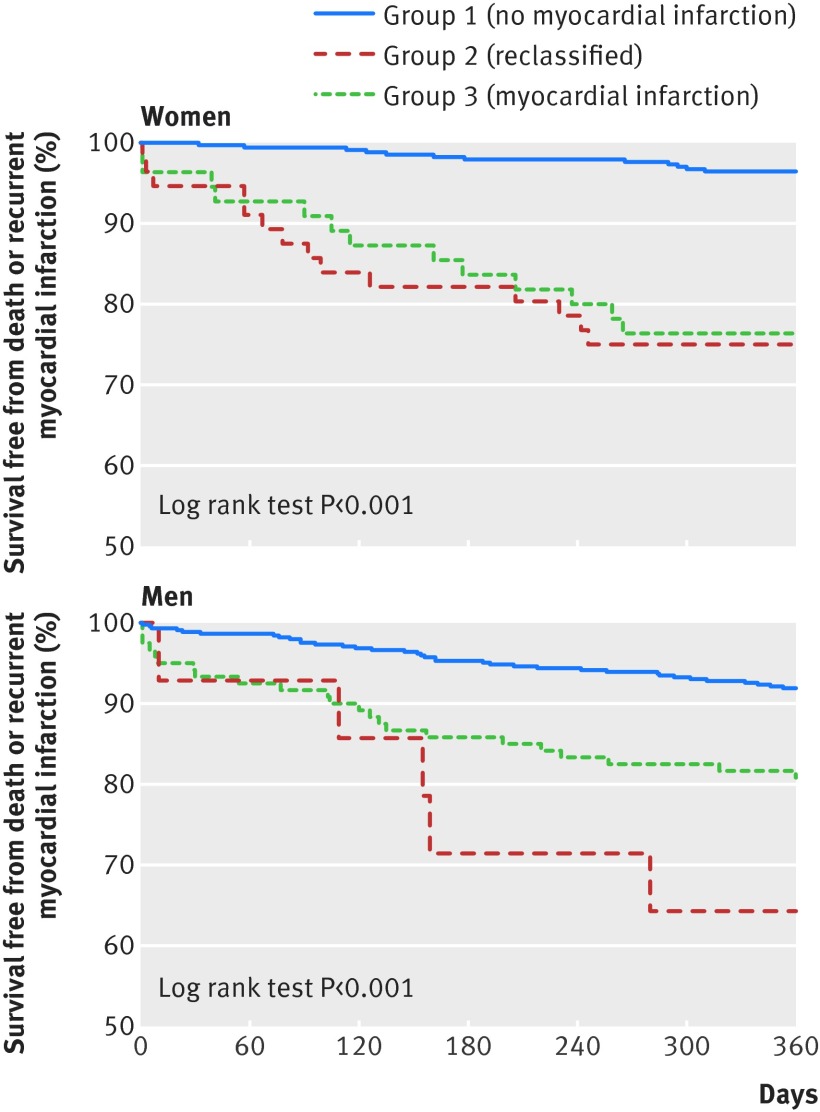
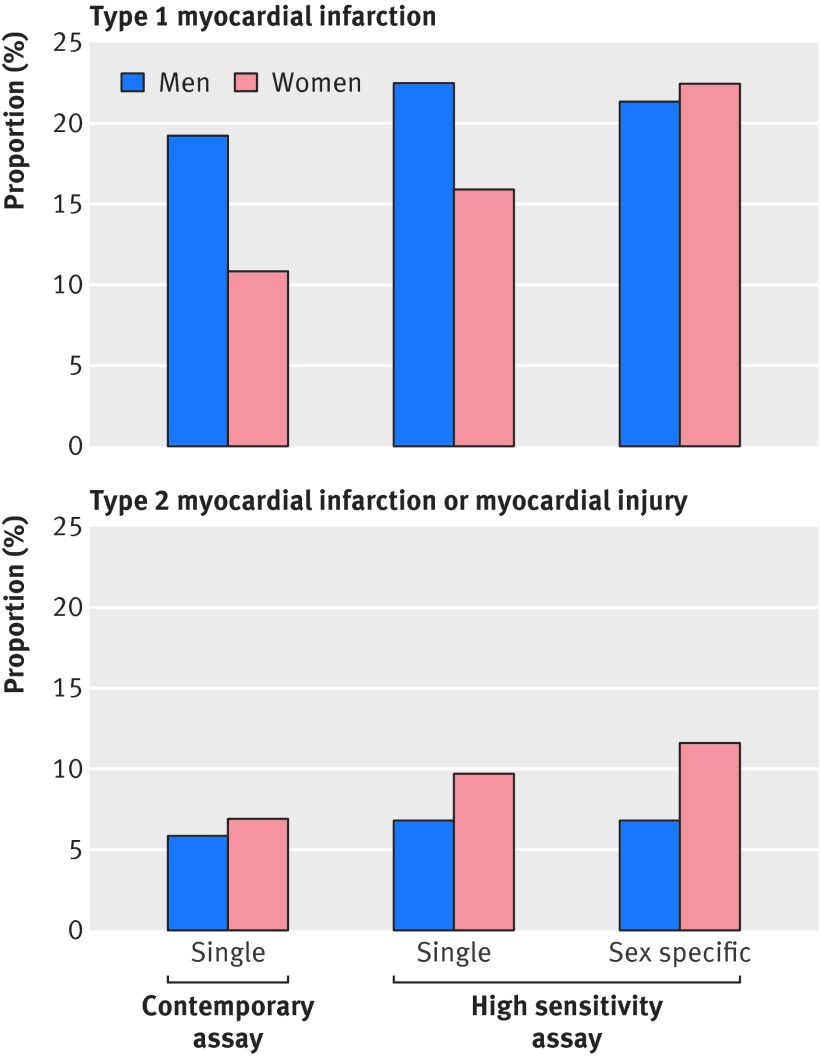
The high sensitivity troponin I assay noticeably increased the diagnosis of myocardial infarction in women (from 11% to 22%; P<0.001) but had a minimal effect in men (from 19% to 21%, P=0.002). Women were less likely than men to be referred to a cardiologist or undergo coronary revascularisation (P<0.05 for both). At 12 months, women with undisclosed increases in troponin concentration (17-49 ng/L) and those with myocardial infarction (≥50 ng/L) had the highest rate of death or reinfarction compared with women without (≤16 ng/L) myocardial infarction (25%, 24%, and 4%, respectively; P<0.001).
Although having little effect in men, a high sensitivity troponin assay with sex specific diagnostic thresholds may double the diagnosis of myocardial infarction in women and identify those at high risk of reinfarction and death. Whether use of sex specific diagnostic thresholds will improve outcomes and tackle inequalities in the treatment of women with suspected acute coronary syndrome requires urgent attention.
采用高敏肌钙蛋白I检测法及针对男性和女性的性别特异性诊断阈值,评估疑似急性冠状动脉综合征患者的心肌梗死诊断情况。
前瞻性队列研究。
英国地区心脏中心。
连续入选的疑似急性冠状动脉综合征患者(n = 1126,46%为女性)。两名心脏病专家使用具有性别特异性诊断阈值(男性34 ng/L,女性16 ng/L)的高敏肌钙蛋白I检测法独立判定心肌梗死诊断,并与当前使用当代检测法(50 ng/L,单一阈值)指导治疗的做法进行比较。
心肌梗死诊断。
高敏肌钙蛋白I检测法显著增加了女性心肌梗死的诊断率(从11%增至22%;P<0.001),但对男性影响极小(从19%增至21%,P = 0.002)。女性被转诊至心脏病专家处或接受冠状动脉血运重建的可能性低于男性(两者P均<0.05)。在12个月时,肌钙蛋白浓度未公开升高(17 - 49 ng/L)的女性和发生心肌梗死(≥50 ng/L)的女性与未发生(≤16 ng/L)心肌梗死的女性相比,死亡或再梗死发生率最高(分别为25%、24%和4%;P<0.001)。
尽管对男性影响不大,但具有性别特异性诊断阈值的高敏肌钙蛋白检测法可能使女性心肌梗死的诊断率翻倍,并识别出再梗死和死亡高风险患者。使用性别特异性诊断阈值是否会改善结局并解决疑似急性冠状动脉综合征女性治疗中的不平等问题,亟待关注。