AlBadri Ahmed, Lai Kha, Wei Janet, Landes Sofy, Mehta Puja K, Li Quanlin, Johnson Delia, Reis Steven E, Kelsey Sheryl F, Bittner Vera, Sopko George, Shaw Leslee J, Pepine Carl J, Bairey Merz C Noel
Barbra Streisand Women's Heart Center, Cedars-Sinai Heart Institute, Los Angeles, California, United States of America.
Biostatistics and Bioinformatics Research Center, Cedars-Sinai Medical Center, Los Angeles, California, United States of America.
PLoS One. 2017 May 19;12(5):e0177684. doi: 10.1371/journal.pone.0177684. eCollection 2017.
Women with signs and symptoms of ischemia, no obstructive coronary artery disease (CAD) and preserved left ventricular ejection fraction (EF) often have diastolic dysfunction and experience elevated rates of major adverse cardiac events (MACE), including heart failure (HF) hospitalization with preserved ejection fraction (HFpEF). We evaluated the predictive value of inflammatory biomarkers for long-term HF hospitalization and all-cause mortality in these women.
We performed a cross-sectional analysis to investigate the relationships between inflammatory biomarkers [serum interleukin-6 (IL-6), C-reactive protein (hs-CRP) and serum amyloid A (SAA)] and median of 6 years follow-up for all-cause mortality and HF hospitalization among women with signs and symptoms of ischemia, non-obstructive CAD and preserved EF. Multivariable Cox regression analysis tested associations between biomarker levels and adverse outcomes.
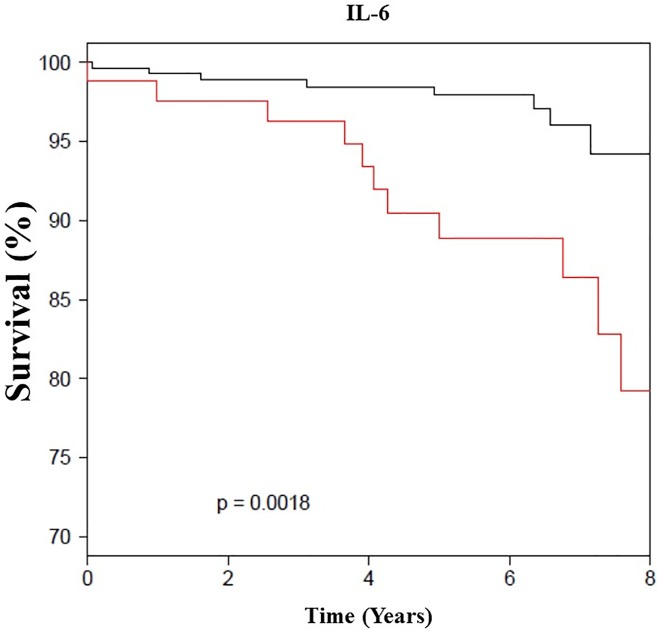
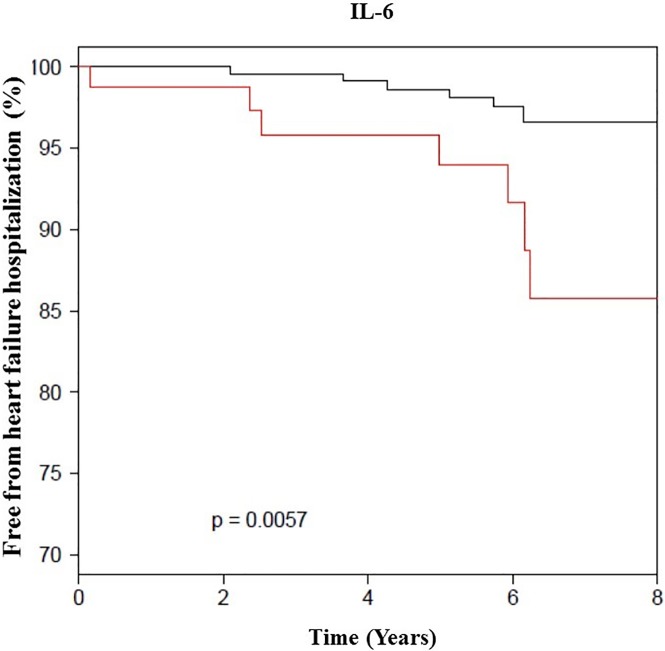
Among 390 women, mean age 56 ± 11 years, median follow up of 6 years, we observed that there is continuous association between IL-6 level and HF hospitalization (adjusted hazard ratio [AHR] 2.5 [1.2-5.0], p = 0.02). In addition, we found significant association between IL-6, SAA levels and all-cause mortality AHR (1.8 [1.1-3.0], p = 0.01) (1.5 [1.0-2.1], p = 0.04), respectively.
In women with signs and symptoms of ischemia, non-obstructive CAD and preserved EF, elevated IL-6 predicted HF hospitalization and all-cause mortality, while SAA level was only associated with all-cause mortality. These results suggest that inflammation plays a role in the pathogenesis of development of HFpEF, as well all-cause mortality.
有缺血症状和体征、无阻塞性冠状动脉疾病(CAD)且左心室射血分数(EF)保留的女性通常存在舒张功能障碍,且发生主要不良心脏事件(MACE)的几率升高,包括射血分数保留的心力衰竭(HF)住院(HFpEF)。我们评估了炎症生物标志物对这些女性长期HF住院和全因死亡率的预测价值。
我们进行了一项横断面分析,以研究炎症生物标志物[血清白细胞介素-6(IL-6)、C反应蛋白(hs-CRP)和血清淀粉样蛋白A(SAA)]与有缺血症状和体征、非阻塞性CAD且EF保留的女性全因死亡率和HF住院6年随访中位数之间的关系。多变量Cox回归分析测试了生物标志物水平与不良结局之间的关联。
在390名平均年龄为56±11岁、中位随访6年的女性中,我们观察到IL-6水平与HF住院之间存在持续关联(调整后风险比[AHR]为2.5[1.2 - 5.0],p = 0.02)。此外,我们分别发现IL-6、SAA水平与全因死亡率AHR之间存在显著关联(分别为1.8[1.1 - 3.0],p = 0.01)(1.5[1.0 - 2.1],p = 0.04)。
在有缺血症状和体征、非阻塞性CAD且EF保留的女性中,IL-6升高可预测HF住院和全因死亡率,而SAA水平仅与全因死亡率相关。这些结果表明,炎症在HFpEF的发病机制以及全因死亡率中起作用。