Lummus Seth C, Donson Andrew M, Gowan Katherine, Jones Kenneth L, Vibhakar Rajeev, Foreman Nicholas K, Kleinschmidt-DeMasters B K
Department of Pathology, The University of Colorado School of Medicine, Aurora, Colorado.
Children's Hospital Colorado, Aurora, Colorado.
Pediatr Blood Cancer. 2017 Dec;64(12). doi: 10.1002/pbc.26656. Epub 2017 May 26.
Posterior fossa (PF) ependymomas (EPNs) in infants less than 1 year of age (iEPN-PF) have a poorer clinical outcome than EPNs in older children. While radiation therapy is the standard of care for the latter, it is withheld in infants to avoid neurotoxicity to immature brain. It is unknown whether the adverse outcome in iEPN-PFs is due to treatment differences or aggressive biology. We examined this question using molecular profiling.
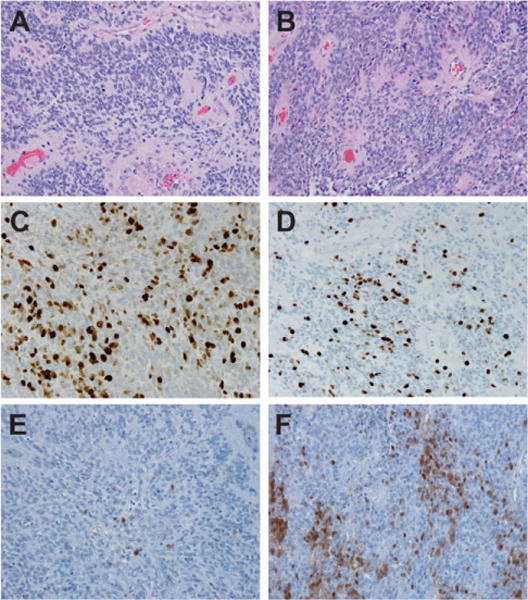
Six anaplastic iEPN-PFs were subjected to transcriptomic analysis and FISH for p16 loss and gains of 1q, and compared with anaplastic PF EPNs from older children. Results were validated by immunohistochemistry (IHC).
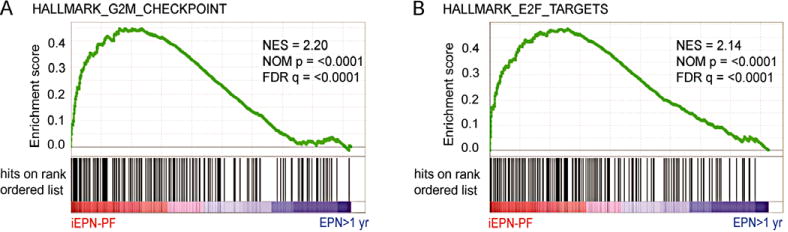
All six iEPN-PFs were grouped within EPN PF subgroup A (PFA). E2F targets and G2M checkpoint were identified as the most enriched gene sets in iEPN-PF, which was validated in a larger independent cohort. Accordingly, MIB-1 IHC demonstrated a higher mitotic rate in iEPN-PFs than noninfant anaplastic EPN PFA. Genetic and protein analyses demonstrated that p16 loss and low p16 protein expression is a hallmark of iEPN-PF, and that none harbored 1q gains. Kaplan-Meier analysis confirmed the poorer clinical outcome of the iEPN-PF cohort.
Biological differences, characterized by loss of p16 expression without gains of 1q in iEPN-PFs, as well as deregulated E2F target gene transcription, are indicative of deregulated p16-CDK4/6-pRB-E2F pathway activity. This may underlie the poor clinical outcome seen in this group of iEPN-PFs, rather than the withholding of radiation therapy. Results suggest a potential actionable therapy for iEPN-PF, namely cyclin-dependent kinase 4/6 (CDK4/6) inhibitors.
1岁以下婴儿的后颅窝(PF)室管膜瘤(EPNs,iEPN-PF)的临床预后比大龄儿童的EPNs更差。虽然放射治疗是大龄儿童EPNs的标准治疗方法,但婴儿不进行放疗以避免对未成熟脑产生神经毒性。iEPN-PFs的不良预后是由于治疗差异还是侵袭性生物学特性尚不清楚。我们使用分子谱分析来研究这个问题。
对6例间变性iEPN-PFs进行转录组分析和FISH检测p16缺失及1q增益情况,并与大龄儿童的间变性PF EPNs进行比较。结果通过免疫组织化学(IHC)验证。
所有6例iEPN-PFs均归入EPN PF A亚组(PFA)。E2F靶点和G2M检查点被确定为iEPN-PF中最富集的基因集,这在一个更大的独立队列中得到验证。相应地,MIB-1 IHC显示iEPN-PFs的有丝分裂率高于非婴儿间变性EPN PFA。基因和蛋白质分析表明,p16缺失和低p16蛋白表达是iEPN-PF的一个标志,且无一例有1q增益。Kaplan-Meier分析证实了iEPN-PF队列较差的临床预后。
iEPN-PFs的生物学差异表现为p16表达缺失且无1q增益,以及E2F靶基因转录失调,这表明p16-CDK4/6-pRB-E2F信号通路活性失调。这可能是该组iEPN-PFs临床预后较差的原因,而非未进行放射治疗。结果提示iEPN-PF可能有一种可行的治疗方法,即细胞周期蛋白依赖性激酶4/6(CDK4/6)抑制剂。