Sawayama Hiroshi, Miyanari Nobutomo, Sugihara Hidetaka, Iwagami Shiro, Mizumoto Takao, Kubota Tatsuo, Haga Yoshio, Baba Hideo
Department of Surgery, National Hospital Organization Kumamoto Medical Center, 1-5 Ninomaru, Kumamoto, 860-0008, Japan.
Department of Gastroenterological Surgery, Graduate School of Medical Sciences, Kumamoto University, 1-1-1 Honjo, Kumamoto, 860-8556, Japan.
Surg Case Rep. 2017 Dec;3(1):74. doi: 10.1186/s40792-017-0350-y. Epub 2017 May 26.
Fournier gangrene due to advanced rectal cancer is a rapidly progressive gangrene of the perineum and buttocks. Emergency surgical debridement of necrotic tissue is crucial, and secondary surgery to resect tumors is necessary for wound healing. However, pelvic exenteration damages the pelvic floor, increasing the likelihood of herniation of internal organs into the infectious wound. The management of pelvic exenteration for rectal cancer with Fournier gangrene has not yet been established. We herein describe the use of a fascia lata free flap in pelvic exenteration for rectal cancer with Fournier gangrene.
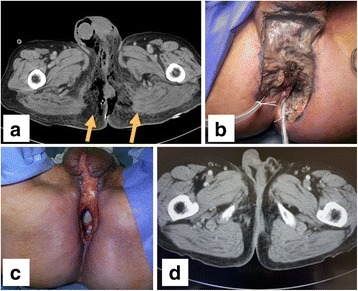
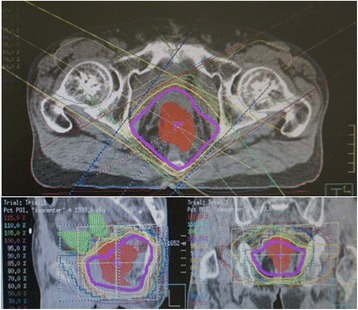
A 66-year-old male who had undergone colostomy for large bowel obstruction due to advanced rectal cancer and continued chemotherapy was referred to our hospital for Fournier gangrene resulting from chemotherapy. Emergency surgical debridement was performed, and the infectious wound around the rectal cancer was treated with intravenous antibiotic agents postoperatively. However, the tumor was exposed by the wound, and exudate persisted. Pelvic exenteration was performed due to tumor infiltration into the bladder and prostate. Tumor resection resulted in a defect in the pelvic floor. A fascia lata free flap (15 × 9 cm) obtained from the left thigh was fixed to the edge of the peritoneum and ileal conduit to close the defect in the pelvic floor and prevent small bowel herniation into the resected space. There was no intraabdominal inflammation or bowel obstruction postoperatively, and outpatient chemotherapy was continued.
Surgical repair with a fascia lata free flap to close the defect in the pelvic floor led to a good clinical outcome for pelvic exenteration in a patient with Fournier gangrene due to advanced rectal cancer.
晚期直肠癌所致的福尼尔坏疽是一种会迅速发展的会阴及臀部坏疽。对坏死组织进行紧急手术清创至关重要,而切除肿瘤的二期手术对于伤口愈合是必要的。然而,盆腔脏器清除术会损害盆底,增加内脏器官疝入感染伤口的可能性。晚期直肠癌合并福尼尔坏疽的盆腔脏器清除术的治疗方法尚未确立。我们在此描述了阔筋膜游离皮瓣在晚期直肠癌合并福尼尔坏疽的盆腔脏器清除术中的应用。
一名66岁男性,因晚期直肠癌导致大肠梗阻接受了结肠造口术,并持续进行化疗,因化疗引发福尼尔坏疽被转诊至我院。进行了紧急手术清创,术后对直肠癌周围的感染伤口使用静脉抗生素进行治疗。然而,肿瘤因伤口暴露,渗出物持续存在。由于肿瘤浸润至膀胱和前列腺,遂进行了盆腔脏器清除术。肿瘤切除导致盆底出现缺损。从左大腿获取一块阔筋膜游离皮瓣(15×9厘米),将其固定于腹膜边缘和回肠造口,以封闭盆底缺损,防止小肠疝入切除空间。术后未出现腹腔内炎症或肠梗阻,继续进行门诊化疗。
对于晚期直肠癌合并福尼尔坏疽的患者,采用阔筋膜游离皮瓣进行手术修复以封闭盆底缺损,在盆腔脏器清除术中取得了良好的临床效果。