Tong Zhou, Liu Lulu, Zheng Yi, Jiang Weiqin, Zhao Peng, Fang Weijia, Wang Weilin
Cancer Biotherapy Center, First Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, China.
Key Laboratory of Precision Diagnosis and Treatment for Hepatobiliary and Pancreatic Tumor of Zhejiang Province, Hangzhou, 310003, China.
World J Surg Oncol. 2017 May 30;15(1):108. doi: 10.1186/s12957-017-1169-5.
Neutrophil-to-lymphocyte ratio (NLR) is one of the systemic inflammation markers, which has prognostic values in many types of tumor. However, hardly any research has reported the relationship between NLR and pancreatic neuroendocrine tumors (PanNETs). In this study, we aimed to evaluate the predictive value of the preoperative peripheral blood NLR on the clinical outcomes in patients of resectable PanNETs.
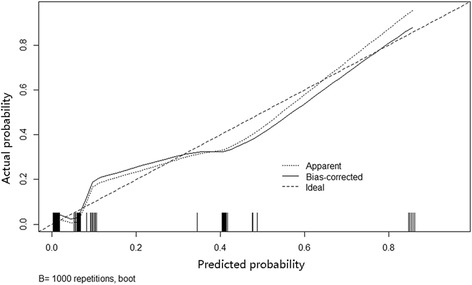
Ninety-five cases of PanNETs registered in the First Affiliated Hospital of Zhejiang University between March 2009 and May 2016 and underwent pancreatic surgery were included in this study. Univariate and multivariate analyses were applied to identify the prognostic factors for PanNETs. Prognostic nomogram and its calibration curve then used R (version 3.3.2) to predict lymph node (LN) metastasis.
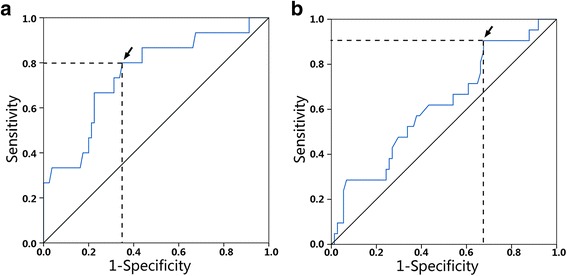
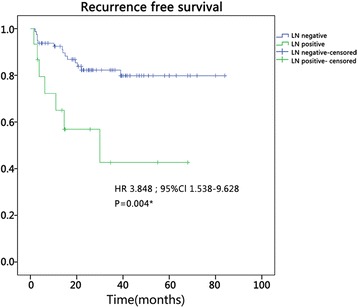
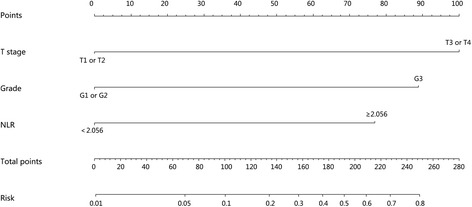
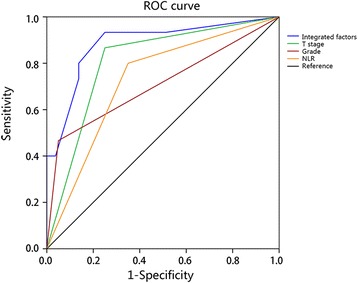
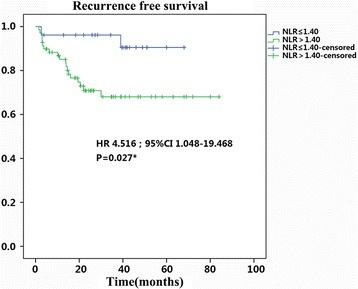
Among these 95 patients, 52 (54.7%) patients were diagnosed as grade 1 (G1) NET (mitotic count <2/10 HPF, Ki-67 ≤2%), 32 (33.7%) as G2 NET (mitotic count 2-20/10 HPF, Ki-67 3-20%), and 11 (11.6%) as G3 NEC (mitotic count >20/10 HPF, Ki-67 >20%). Increased NLR was found to relate with advanced T stage, LN metastasis, tumor thrombus formation, and advanced grade (p < 0.05 for all). Multivariate logistic regression was performed and indicated that NLR (HR 6.74; p = 0.02) was an independent prognostic factor for LN metastasis. Furthermore, we developed a nomogram based on the combination of NLR, T stage, and grade for LN metastasis with a good discrimination ability with the AUC (area under the curve) of 0.885. This nomogram showed larger AUC than those using NLR (0.725), T stage (0.808), or grade (0.708) alone as a prognostic factor, which means this system achieved a more optional performance in predicting clinical outcomes. Finally, the Kaplan-Meier curve indicated that the recurrence-free survival (RFS) of patients with high NLR (NLR >1.40, RFS 61.1 ± 4.4 months) decreased significantly as compared with those of low NLR (NLR ≤1.40, RFS 63.8 ± 2.9 month, p < 0.05).
The preoperative NLR is a potential independent predictor for LN metastasis and RFS. Our nomogram highlighted the important role of NLR in prognosis, which might be considered as a convenient indicator for lymph node metastasis, especially during the initial diagnosis for resectable PanNETs.
中性粒细胞与淋巴细胞比值(NLR)是全身炎症标志物之一,在多种肿瘤类型中具有预后价值。然而,几乎没有研究报道NLR与胰腺神经内分泌肿瘤(PanNETs)之间的关系。在本研究中,我们旨在评估术前外周血NLR对可切除PanNETs患者临床结局的预测价值。
纳入2009年3月至2016年5月在浙江大学第一附属医院登记并接受胰腺手术的95例PanNETs患者。采用单因素和多因素分析确定PanNETs的预后因素。然后使用R(版本3.3.2)绘制预后列线图及其校准曲线,以预测淋巴结(LN)转移。
在这95例患者中,52例(54.7%)患者被诊断为1级(G1)神经内分泌肿瘤(有丝分裂计数<2/10高倍视野,Ki-67≤2%),32例(33.7%)为G2神经内分泌肿瘤(有丝分裂计数2-20/10高倍视野,Ki-67 3-20%),11例(11.6%)为G3神经内分泌癌(有丝分裂计数>20/10高倍视野,Ki-67>20%)。发现NLR升高与T分期进展、LN转移、肿瘤血栓形成和分级进展相关(所有p<0.05)。进行多因素逻辑回归分析,结果表明NLR(HR 6.74;p=0.02)是LN转移的独立预后因素。此外,我们基于NLR、T分期和分级组合开发了用于预测LN转移的列线图,其具有良好的辨别能力,曲线下面积(AUC)为0.885。该列线图的AUC大于单独使用NLR(0.725)、T分期(0.808)或分级(0.708)作为预后因素时的AUC,这意味着该系统在预测临床结局方面表现更优。最后,Kaplan-Meier曲线表明,高NLR患者(NLR>1.40,无复发生存期[RFS]为61.1±4.4个月)的RFS与低NLR患者(NLR≤1.40,RFS为63.8±2.9个月,p<0.05)相比显著降低。
术前NLR是LN转移和RFS的潜在独立预测指标。我们的列线图突出了NLR在预后中的重要作用,可作为LN转移的便捷指标,尤其是在可切除PanNETs的初始诊断期间。