Stellmann Jan-Patrick, Krumbholz Markus, Friede Tim, Gahlen Anna, Borisow Nadja, Fischer Katrin, Hellwig Kerstin, Pache Florence, Ruprecht Klemens, Havla Joachim, Kümpfel Tania, Aktas Orhan, Hartung Hans-Peter, Ringelstein Marius, Geis Christian, Kleinschnitz Christoph, Berthele Achim, Hemmer Bernhard, Angstwurm Klemens, Young Kim Lea, Schuster Simon, Stangel Martin, Lauda Florian, Tumani Hayrettin, Mayer Christoph, Zeltner Lena, Ziemann Ulf, Linker Ralf Andreas, Schwab Matthias, Marziniak Martin, Then Bergh Florian, Hofstadt-van Oy Ulrich, Neuhaus Oliver, Zettl Uwe, Faiss Jürgen, Wildemann Brigitte, Paul Friedemann, Jarius Sven, Trebst Corinna, Kleiter Ingo
Institut für Neuroimmunologie und Multiple Sklerose (INIMS), Universitätsklinikum Hamburg-Eppendorf, Hamburg, Germany.
Klinik und Poliklinik für Neurologie, Universitätsklinikum Hamburg-Eppendorf, Hamburg, Germany.
J Neurol Neurosurg Psychiatry. 2017 Aug;88(8):639-647. doi: 10.1136/jnnp-2017-315603. Epub 2017 Jun 1.
To analyse predictors for relapses and number of attacks under different immunotherapies in patients with neuromyelitis optica spectrum disorder (NMOSD).
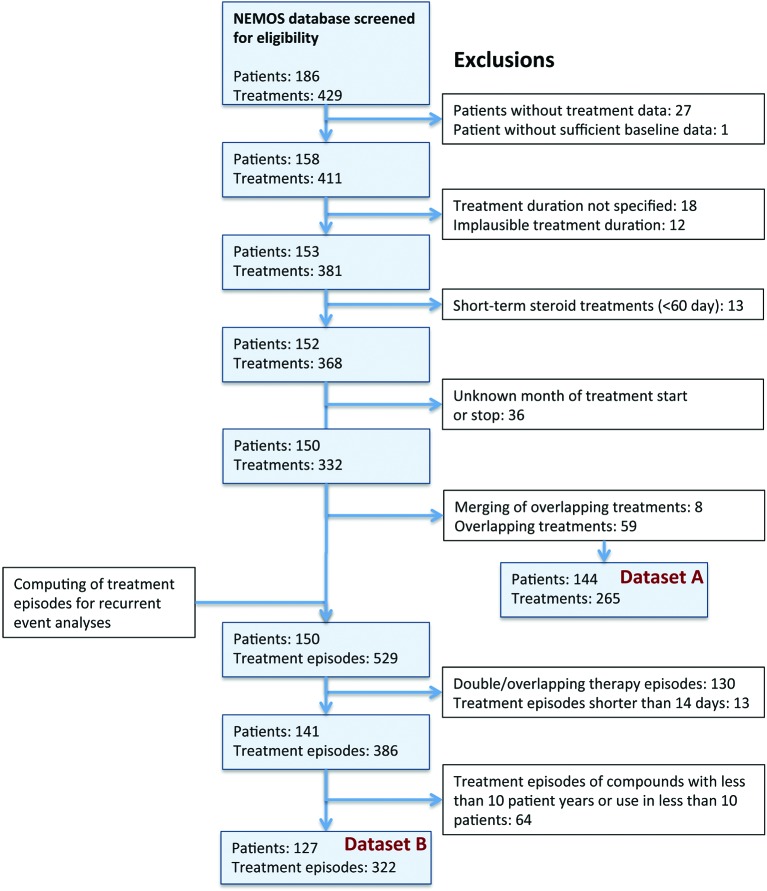
This is a retrospective cohort study conducted in neurology departments at 21 regional and university hospitals in Germany. Eligible participants were patients with aquaporin-4-antibody-positive or aquaporin-4-antibody-negative NMOSD. Main outcome measures were HRs from Cox proportional hazard regression models adjusted for centre effects, important prognostic factors and repeated treatment episodes.
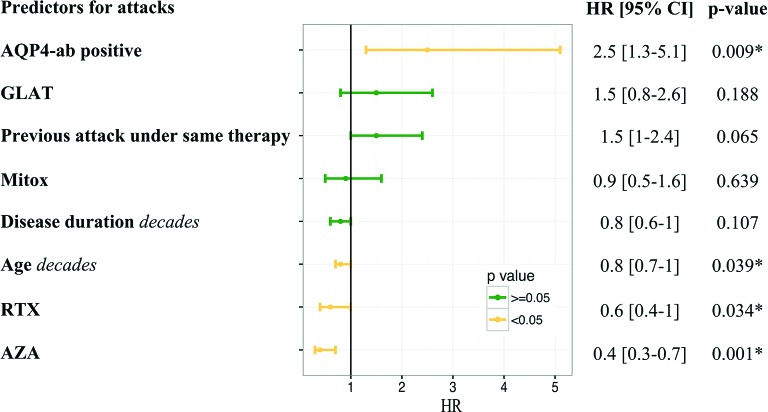
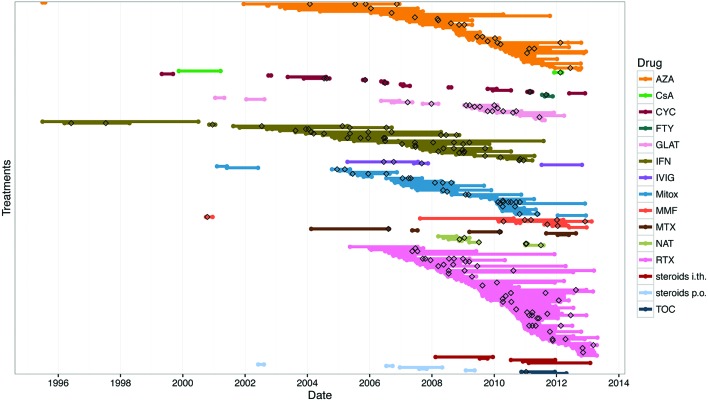
265 treatment episodes with a mean duration of 442 days (total of 321 treatment years) in 144 patients (mean age at first attack: 40.9 years, 82.6% female, 86.1% aquaporin-4-antibody-positive) were analysed. 191 attacks occurred during any of the treatments (annual relapse rate=0.60). The most common treatments were rituximab (n=77, 111 patient-years), azathioprine (n=52, 68 patient-years), interferon-β (n=32, 61 patient-years), mitoxantrone (n=34, 32.1 patient-years) and glatiramer acetate (n=17, 10 patient-years). Azathioprine (HR=0.4, 95% CI 0.3 to 0.7, p=0.001) and rituximab (HR=0.6, 95% CI 0.4 to 1.0, p=0.034) reduced the attack risk compared with interferon-β, whereas mitoxantrone and glatiramer acetate did not. Patients who were aquaporin-4-antibody-positive had a higher risk of attacks (HR=2.5, 95% CI 1.3 to 5.1, p=0.009). Every decade of age was associated with a lower risk for attacks (HR=0.8, 95% CI 0.7 to 1.0, p=0.039). A previous attack under the same treatment tended to be predictive for further attacks (HR=1.5, 95% CI 1.0 to 2.4, p=0.065).
Age, antibody status and possibly previous attacks predict further attacks in patients treated for NMOSD. Azathioprine and rituximab are superior to interferon-β.
分析视神经脊髓炎谱系障碍(NMOSD)患者在不同免疫疗法下复发的预测因素及发作次数。
这是一项在德国21家地区和大学医院神经内科进行的回顾性队列研究。符合条件的参与者为水通道蛋白4抗体阳性或水通道蛋白4抗体阴性的NMOSD患者。主要结局指标是经中心效应、重要预后因素和重复治疗发作调整后的Cox比例风险回归模型的风险比(HR)。
分析了144例患者(首次发作时的平均年龄:40.9岁,82.6%为女性,86.1%为水通道蛋白4抗体阳性)的265个治疗疗程,平均持续时间为442天(总计321个治疗年)。在任何一种治疗期间发生了191次发作(年复发率=0.60)。最常用的治疗方法是利妥昔单抗(n=77,111患者年)、硫唑嘌呤(n=52,68患者年)、干扰素-β(n=32,61患者年)、米托蒽醌(n=34,32.1患者年)和醋酸格拉替雷(n=17,10患者年)。与干扰素-β相比,硫唑嘌呤(HR=0.4,95%CI 0.3至0.7,p=0.001)和利妥昔单抗(HR=0.6,95%CI 0.4至1.0,p=0.034)降低了发作风险,而米托蒽醌和醋酸格拉替雷则没有。水通道蛋白4抗体阳性的患者发作风险更高(HR=2.5,95%CI 1.3至5.1,p=0.009)。每增长十岁发作风险降低(HR=0.8,95%CI 0.7至1.0,p=0.039)。在相同治疗下之前有过发作往往可预测进一步发作(HR=1.5,95%CI 1.0至2.4,p=0.065)。
年龄、抗体状态以及可能之前的发作可预测接受NMOSD治疗患者的进一步发作。硫唑嘌呤和利妥昔单抗优于干扰素-β。