Terrier Jean E, Mulhall John P, Nelson Christian J
Male Sexual and Reproductive Medicine Program, Urology Service, Department of Surgery, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
Department of Psychiatry and Behavioral Sciences, Memorial Sloan Kettering Cancer Center, New York, NY, USA.
J Sex Med. 2017 Jun;14(6):804-809. doi: 10.1016/j.jsxm.2017.04.672.
The International Index of Erectile Function (IIEF) is the gold standard validated instrument for defining erectile function (EF) and its response to treatment. The EF domain (EFD) contains six questions and is a sensitive and specific measurement of treatment-related changes in EF. The EFD score has been widely used as a primary assessment end point for clinical trials of EF recovery after radical prostatectomy (RP). Various EFD scores have been used to define functional erections. Recently, an EFD score of at least 22 has been used as a threshold in major post-RP penile rehabilitation studies.
To define the EFD score that optimally defines "functional" erections after RP.
We assessed men 24 months after RP using the IIEF and specifically analyzed the scores of the EFD and intercourse satisfaction domain (ISD).
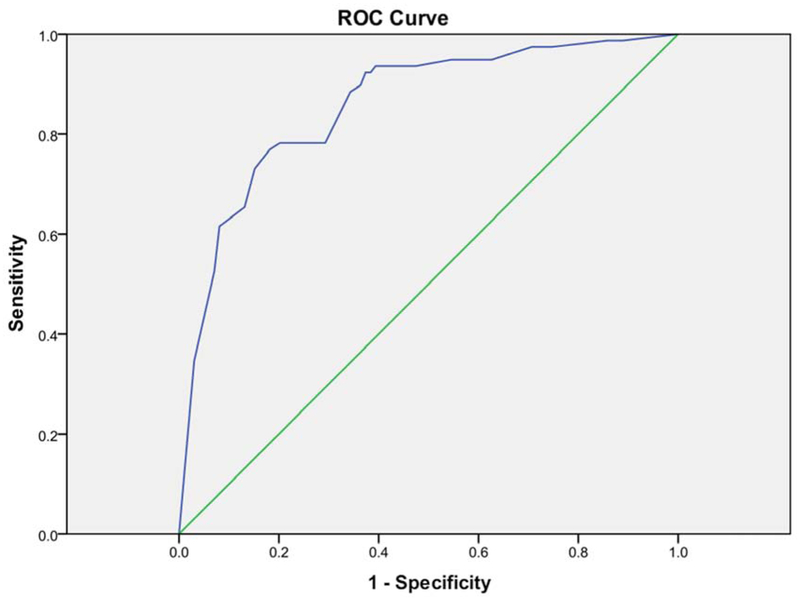
We used two questions on satisfaction (score = 0-5) and enjoyment (score = 0-5) from the ISD to classify IS (score = 0-10). We tested the following intercourse satisfaction classifications: ISD score equal to 10, ISD score of at least 8, and a score of at least 4 for the ISD questions on satisfaction and enjoyment. We used the classification that produced the largest area under the curve (AUC) using a receiver operating characteristic (ROC) curve. Then, we used a three-step process to determine the optimal EFD score cutoff using sensitivity and specificity analysis.
One hundred seventy-eight men had an average age at RP of 58 ± 7 years and a 24-month EFD score of 20 ± 9. Sixty-four percent had complete nerve-sparing surgery, 35% had partial nerve-sparing surgery, and 1% had the nerves fully resected. Thirty-three percent had laparoscopic RP and 67% had open RP. The ROC curves produced AUCs of 0.80 (ISD score = 10), 0.85 (ISD score ≥ 8), and 0.86 (ISD scores for satisfaction and enjoyment ≥ 4; P < .001 for all comparisons). Using the IS criterion of ISD scores for satisfaction and enjoyment of at least 4 (largest AUC), the sensitivity and specificity values were 0.89 and 0.66 for an ESD score equal to 22, 0.78 and 0.71 for a score equal to 23, 0.78 and 0.80 for a score equal to 24, 0.77 and 0.82 for a score equal to 25, and 0.73 and 0.85 for a score equal to 26. The scores of 24 and 25 met the criteria outlined in the first two steps of analysis. The score of 24 was selected as the cutoff using face valid judgment and the previous literature.
These data support an EFD score of 24 as a valid cutoff defining "functional" erection in men with erectile dysfunction after RP. These data are important for clinicians in counseling patients and to researchers to define inclusion criteria and treatment end points for trials of erectile dysfunction after RP. Terrier JE, Muhall JP, Nelson CJ. Exploring the Optimal Erectile Function Domain Score Cutoff That Defines Sexual Satisfaction After Radical Prostatectomy. J Sex Med 2017;14:804-809.
国际勃起功能指数(IIEF)是用于定义勃起功能(EF)及其对治疗反应的经过验证的金标准工具。勃起功能领域(EFD)包含六个问题,是对与治疗相关的勃起功能变化的敏感且特异的测量方法。EFD评分已被广泛用作前列腺癌根治术(RP)后勃起功能恢复临床试验的主要评估终点。各种EFD评分已被用于定义功能性勃起。最近,在主要的RP后阴茎康复研究中,EFD评分至少为22被用作一个阈值。
确定能最佳定义RP后“功能性”勃起的EFD评分。
我们使用IIEF对RP后24个月的男性进行评估,并特别分析了EFD和性交满意度领域(ISD)的评分。
我们使用ISD中关于满意度(评分=0-5)和愉悦度(评分=0-5)的两个问题来对性交满意度(IS)进行分类(评分=0-10)。我们测试了以下性交满意度分类:ISD评分等于10、ISD评分至少为8,以及ISD中关于满意度和愉悦度的问题评分至少为4。我们使用产生最大曲线下面积(AUC)的分类,通过受试者工作特征(ROC)曲线进行分析。然后,我们使用三步法通过敏感性和特异性分析来确定最佳的EFD评分临界值。
178名男性在RP时的平均年龄为58±7岁,24个月时的EFD评分为20±9。64%的患者接受了完全保留神经的手术,35%的患者接受了部分保留神经的手术,1%的患者神经被完全切除。33%的患者接受了腹腔镜RP,67%的患者接受了开放性RP。ROC曲线产生的AUC分别为0.80(ISD评分=10)、0.85(ISD评分≥8)和0.86(ISD中关于满意度和愉悦度的评分≥4;所有比较的P<0.001)。使用ISD中关于满意度和愉悦度评分至少为4的IS标准(最大AUC),当ESD评分为22时,敏感性和特异性值分别为0.89和0.66;评分为23时,分别为0.78和0.71;评分为24时,分别为0.78和0.80;评分为25时,分别为0.77和0.82;评分为26时,分别为0.73和0.85。24分和25分符合分析前两步中概述的标准。根据表面效度判断和先前的文献,选择24分作为临界值。
这些数据支持将EFD评分24作为定义RP后勃起功能障碍男性“功能性”勃起的有效临界值。这些数据对于临床医生为患者提供咨询以及研究人员确定RP后勃起功能障碍试验的纳入标准和治疗终点具有重要意义。特里尔JE,穆哈尔JP,纳尔逊CJ。探索定义前列腺癌根治术后性满意度的最佳勃起功能领域评分临界值。《性医学杂志》2017;14:804-809。