Axell Richard G, Giblett Joel P, White Paul A, Klein Andrew, Hampton-Til James, O'Sullivan Michael, Braganza Denise, Davies William R, West Nick E J, Densem Cameron G, Hoole Stephen P
Medical Physics and Clinical Engineering, Cambridge University Hospital NHS Foundation Trust, Cambridge, United Kingdom.
Postgraduate Medical Institute, Anglia Ruskin University, Chelmsford, United Kingdom.
J Am Heart Assoc. 2017 Jun 6;6(6):e005820. doi: 10.1161/JAHA.117.005820.
We sought to determine whether right ventricular stunning could be detected after supply (during coronary balloon occlusion [BO]) and supply/demand ischemia (induced by rapid pacing [RP] during transcatheter aortic valve replacement) in humans.
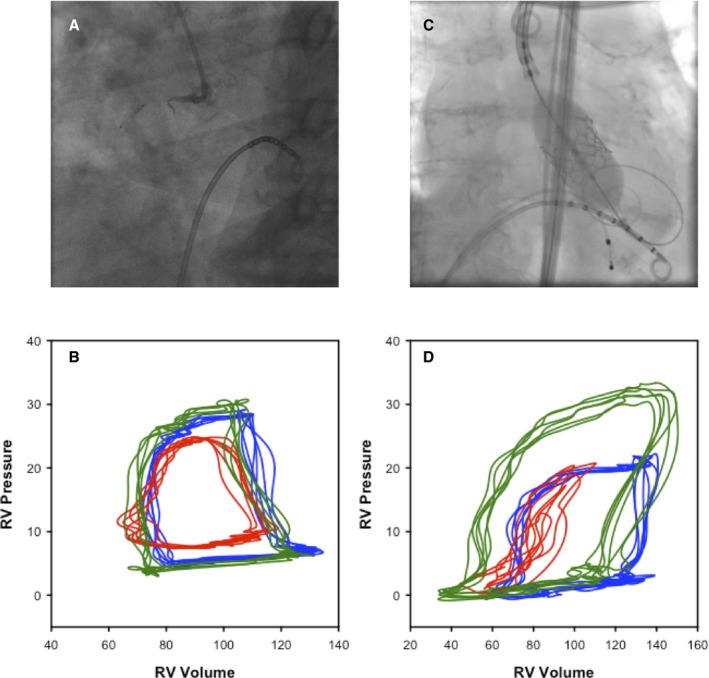
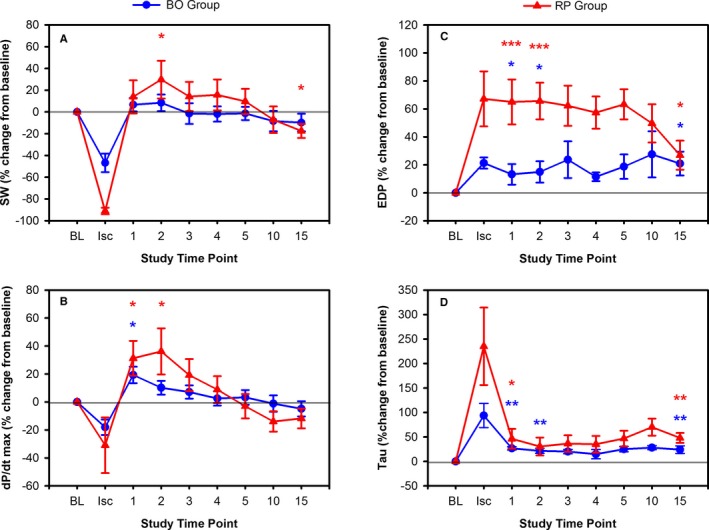
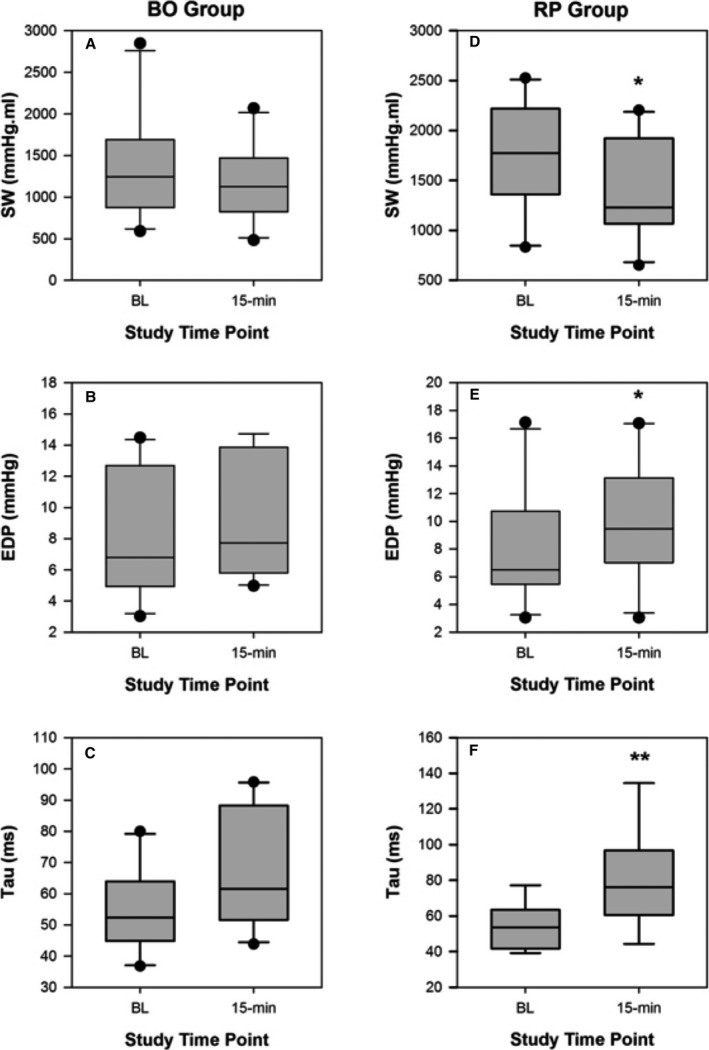
Ten subjects with single-vessel right coronary artery disease undergoing percutaneous coronary intervention with normal ventricular function were studied in the BO group. Ten subjects undergoing transfemoral transcatheter aortic valve replacement were studied in the RP group. In both, a conductance catheter was placed into the right ventricle, and pressure volume loops were recorded at baseline and for intervals over 15 minutes after a low-pressure BO for 1 minute or a cumulative duration of RP for up to 1 minute. Ischemia-induced diastolic dysfunction was seen 1 minute after RP (end-diastolic pressure [mm Hg]: 8.1±4.2 versus 12.1±4.1, <0.001) and BO (end-diastolic pressure [mm Hg]: 8.14.0 versus 8.7±4.0, =0.03). Impairment of systolic and diastolic function after BO remained at 15-minutes recovery (ejection fraction [%]: 55.7±9.0 versus 47.8±6.3, <0.01; end-diastolic pressure [mm Hg]: 8.1±4.0 versus 9.2±3.9, <0.01). Persistent diastolic dysfunction was also evident in the RP group at 15-minutes recovery (end-diastolic pressure [mm Hg]: 8.1±4.1 versus 9.9±4.4, =0.03) and there was also sustained impairment of load-independent indices of systolic function at 15 minutes after RP (end-systolic elastance and ventriculo-arterial coupling [mm Hg/mL]: 1.25±0.31 versus 0.85±0.43, <0.01).
RP and right coronary artery balloon occlusion both cause ischemic right ventricular dysfunction with stunning observed later during the procedure. This may have intraoperative implications in patients without right ventricular functional reserve.
我们试图确定在人体供血(冠状动脉球囊闭塞 [BO] 期间)以及供血/需求性缺血(经导管主动脉瓣置换期间快速起搏 [RP] 诱发)后是否能检测到右心室顿抑。
BO组研究了10名单支右冠状动脉疾病且心室功能正常、正在接受经皮冠状动脉介入治疗的受试者。RP组研究了10名正在接受经股动脉经导管主动脉瓣置换的受试者。两组均将一根电导导管置入右心室,并在基线时以及在1分钟的低压BO或长达1分钟的累计RP持续时间后15分钟内的各个时间段记录压力容积环。RP(舒张末期压力 [mmHg]:8.1±4.2 对比 12.1±4.1,<0.001)和BO(舒张末期压力 [mmHg]:8.1±4.0 对比 8.7±4.0,=0.03)后1分钟可见缺血诱导的舒张功能障碍。BO后收缩和舒张功能的损害在恢复15分钟时仍存在(射血分数 [%]:55.7±9.0 对比 47.8±6.3,<0.01;舒张末期压力 [mmHg]:8.1±4.0 对比 9.2±3.9,<0.01)。RP组在恢复15分钟时持续舒张功能障碍也很明显(舒张末期压力 [mmHg]:8.1±4.1 对比 9.9±4.4,=0.03),并且在RP后15分钟时收缩功能的负荷无关指标也存在持续损害(收缩末期弹性和心室 - 动脉耦合 [mmHg/mL]:1.25±0.31 对比 0.85±0.43,<0.01)。
RP和右冠状动脉球囊闭塞均会导致缺血性右心室功能障碍,并在手术过程后期观察到顿抑。这可能对没有右心室功能储备的患者产生术中影响。