Lindman Brian R, Maniar Hersh S, Jaber Wael A, Lerakis Stamatios, Mack Michael J, Suri Rakesh M, Thourani Vinod H, Babaliaros Vasilis, Kereiakes Dean J, Whisenant Brian, Miller D Craig, Tuzcu E Murat, Svensson Lars G, Xu Ke, Doshi Darshan, Leon Martin B, Zajarias Alan
From the Washington University School of Medicine, St. Louis, MO (B.R.L., H.S.M., A.Z.); Cleveland Clinic Foundation, OH (W.A.J., E.M.T., L.G.S.); Emory University School of Medicine, Atlanta, GA (S.L., V.H.T., V.B.); Baylor Scott and White Health, Plano, TX (M.J.M.); Mayo Clinic, Rochester, MN (R.M.S.); The Christ Hospital Heart and Vascular Center/The Lindner Research Center, Cincinnati, OH (D.J.K.); Intermountain Heart Center, Murray, UT (B.W.); Stanford University School of Medicine, CA (D.C.M.); Cardiovascular Research Foundation, New York, NY (K.X., M.B.L.); and Columbia University Medical Center/New York Presbyterian Hospital (D.D., M.B.L.).
Circ Cardiovasc Interv. 2015 Apr;8(4). doi: 10.1161/CIRCINTERVENTIONS.114.002073.
Tricuspid regurgitation (TR) and right ventricular (RV) dysfunction adversely affect outcomes in patients with heart failure or mitral valve disease, but their impact on outcomes in patients with aortic stenosis treated with transcatheter aortic valve replacement has not been well characterized.
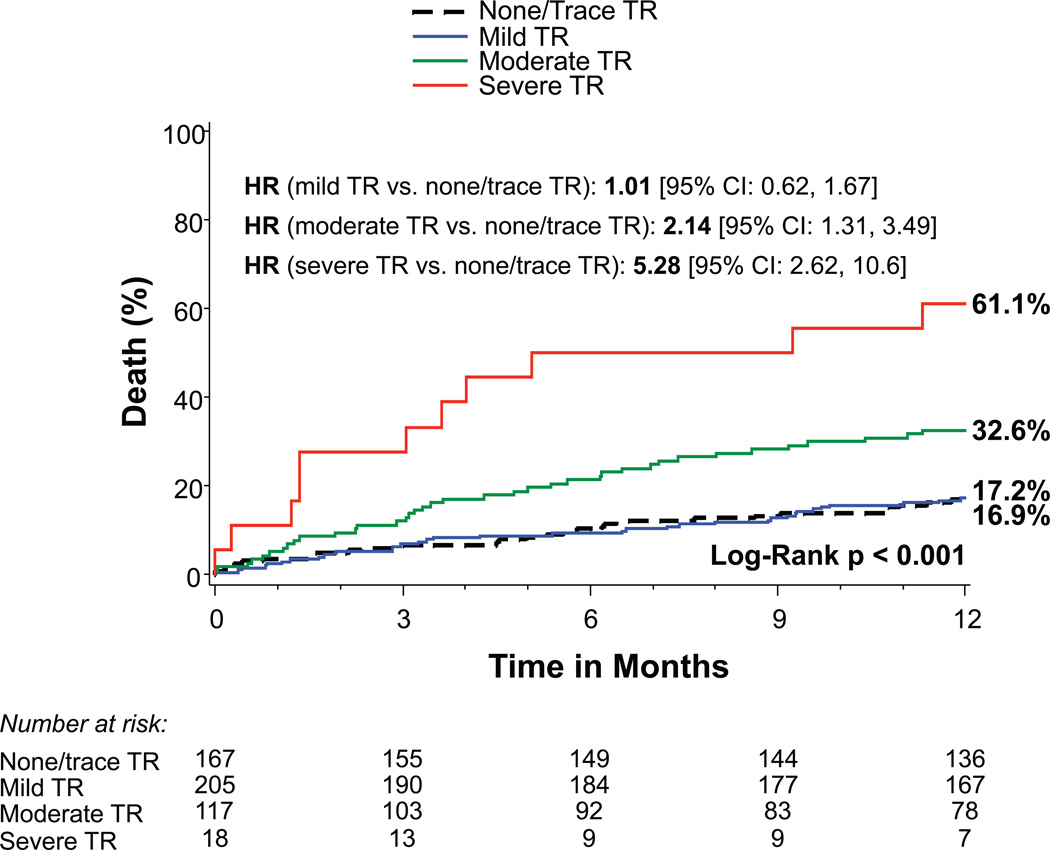
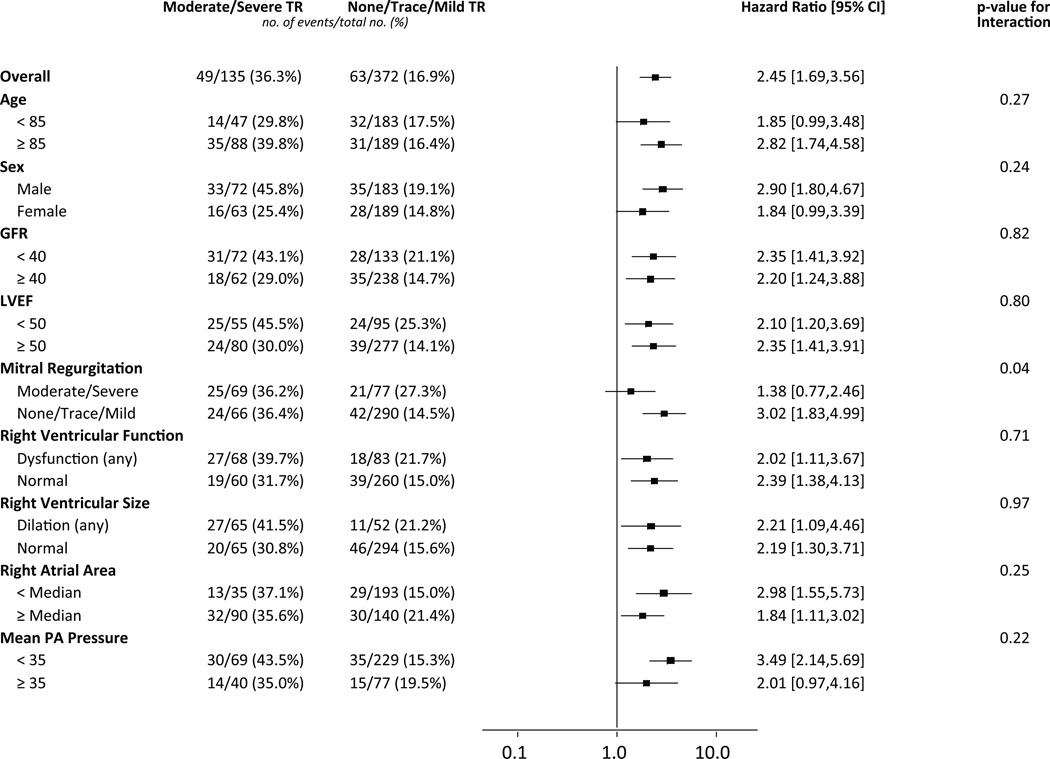
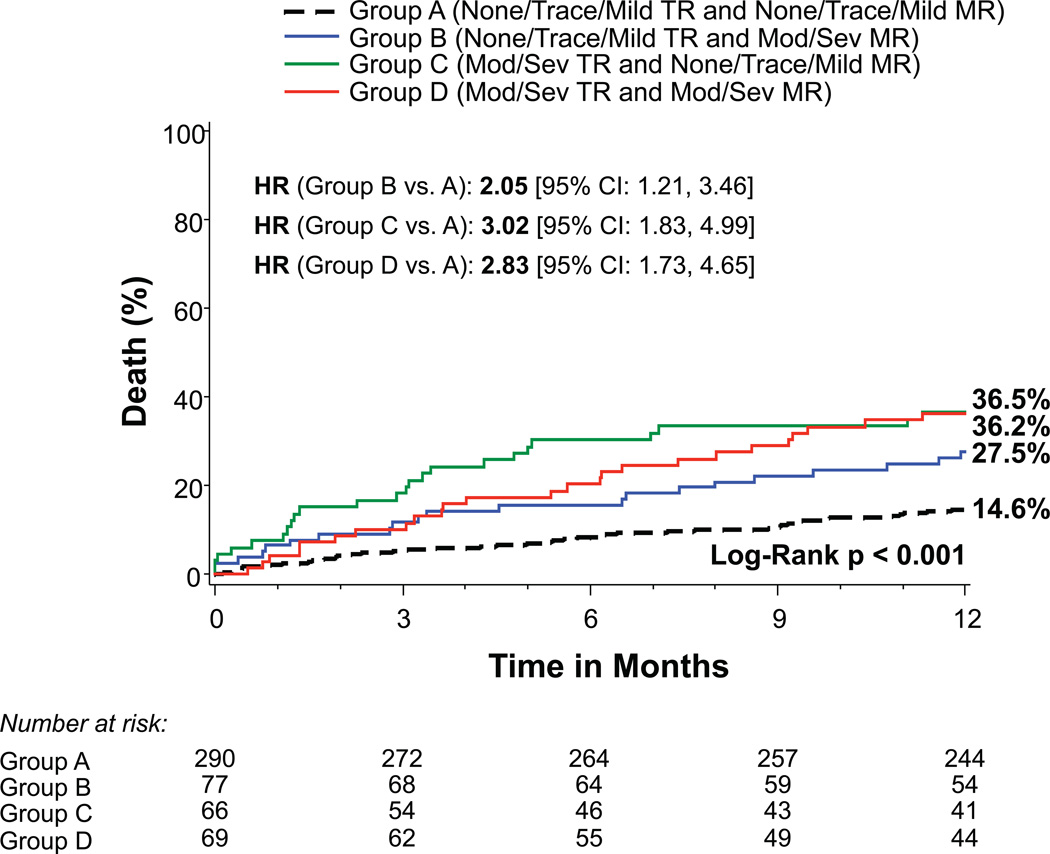
Among 542 patients with symptomatic aortic stenosis treated in the Placement of Aortic Transcatheter Valves (PARTNER) II trial (inoperable cohort) with a Sapien or Sapien XT valve via a transfemoral approach, baseline TR severity, right atrial and RV size and RV function were evaluated by echocardiography according to established guidelines. One-year mortality was 16.9%, 17.2%, 32.6%, and 61.1% for patients with no/trace (n=167), mild (n=205), moderate (n=117), and severe (n=18) TR, respectively (P<0.001). Increasing severity of RV dysfunction as well as right atrial and RV enlargement were also associated with increased mortality (P<0.001). After multivariable adjustment, severe TR (hazard ratio, 3.20; 95% confidence interval, 1.50-6.82; P=0.003) and moderate TR (hazard ratio, 1.60; 95% confidence interval, 1.02-2.52; P=0.042) remained associated with increased mortality as did right atrial and RV enlargement, but not RV dysfunction. There was an interaction between TR and mitral regurgitation severity (P=0.04); the increased hazard of death associated with moderate/severe TR only occurred in those with no/trace/mild mitral regurgitation.
In inoperable patients treated with transcatheter aortic valve replacement, moderate or severe TR and right heart enlargement are independently associated with increased 1-year mortality; however, the association between moderate or severe TR and an increased hazard of death was only found in those with minimal mitral regurgitation at baseline. These findings may improve our assessment of anticipated benefit from transcatheter aortic valve replacement and support the need for future studies on TR and the right heart, including whether concomitant treatment of TR in operable but high-risk patients with aortic stenosis is warranted.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT01314313.
三尖瓣反流(TR)和右心室(RV)功能障碍对心力衰竭或二尖瓣疾病患者的预后产生不利影响,但其对经导管主动脉瓣置换术治疗的主动脉瓣狭窄患者预后的影响尚未得到充分描述。
在经股动脉途径使用Sapien或Sapien XT瓣膜治疗有症状主动脉瓣狭窄的542例患者中,纳入经导管主动脉瓣置换术(PARTNER)II试验(不可手术队列),根据既定指南通过超声心动图评估基线TR严重程度、右心房和RV大小以及RV功能。无/微量(n = 167)、轻度(n = 205)、中度(n = 117)和重度(n = 18)TR患者的1年死亡率分别为16.9%、17.2%、32.6%和61.1%(P<0.001)。RV功能障碍严重程度增加以及右心房和RV扩大也与死亡率增加相关(P<0.001)。多变量调整后,重度TR(风险比,3.20;95%置信区间,1.50 - 6.82;P = 0.003)和中度TR(风险比,1.60;95%置信区间,1.02 - 2.52;P = 0.042)与死亡率增加仍然相关,右心房和RV扩大也是如此,但RV功能障碍并非如此。TR与二尖瓣反流严重程度之间存在相互作用(P = 0.04);与中度/重度TR相关的死亡风险增加仅发生在无/微量/轻度二尖瓣反流的患者中。
在接受经导管主动脉瓣置换术的不可手术患者中,中度或重度TR和右心扩大与1年死亡率增加独立相关;然而,中度或重度TR与死亡风险增加之间的关联仅在基线二尖瓣反流最小的患者中发现。这些发现可能会改善我们对经导管主动脉瓣置换术预期获益的评估,并支持未来对TR和右心进行研究的必要性,包括对于可手术但高危的主动脉瓣狭窄患者是否有必要同时治疗TR。