Liver Research Center, Division of Hepatology, Department of Gastroenterology and Hepatology, Chang Gung Memorial Hospital, Taoyuan, Taiwan.
Department of Medicine, College of Medicine, Chang Gung University, Taoyuan, Taiwan.
Sci Rep. 2017 Jun 6;7(1):2881. doi: 10.1038/s41598-017-03096-y.
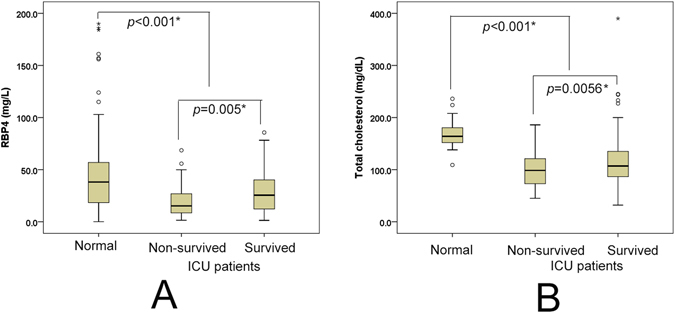
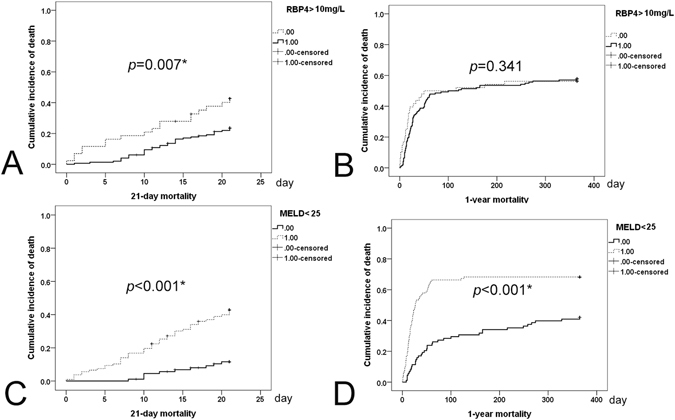
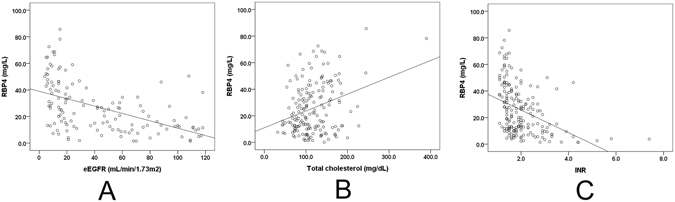
The implications of retinol-binding protein-4 (RBP4) expression in critically ill patients with underlying liver diseases remain unclear. A prospective cohort study involving 200 liver intensive care unit (ICU) patients was conducted, with 274 blood donors as controls. Patient outcomes were assessed using Cox and Kaplan-Meier analyses. Of the 200 ICU patients (mean age: 56.0 yrs), 79.5% were male, 72.5% were cirrhotic, 62% were septic, 29.5% were diabetic, and 29% expired in the ICU (median admission: 7.5 days). ICU patients had lower baseline RBP4 (25.6+/-18.4 vs. 43.8+/-35.0 mg/L, p < 0.001) and total cholesterol (TC) levels than controls. The surviving ICU patients had lower baseline international normalized ratios (INRs) of prothrombin time, model for end-stage liver disease (MELD) scores and sepsis rates, but higher estimated glomerular filtration rates (eGFRs) and RBP4 levels than non-surviving patients. eGFRs, INRs and TC levels were independently associated with RBP4 levels. Only surviving patients exhibited significantly increased RBP4 levels after ICU discharge. Baseline RBP4 levels and MELD scores predicted 21-day (≤10 mg/L) and 1-year (≥25) mortality, respectively. In critically ill patients with underlying liver disease, with a link to eGFRs, INRs and TC levels, the baseline RBP4 may serve as a marker for short-term mortality.
背景不明的基础肝脏疾病危重症患者视黄醇结合蛋白 4(RBP4)的表达意味着什么。进行了一项涉及 200 例肝脏重症监护病房(ICU)患者的前瞻性队列研究,以 274 名献血者作为对照。使用 Cox 和 Kaplan-Meier 分析评估患者的预后。在 200 例 ICU 患者中(平均年龄:56.0 岁),79.5%为男性,72.5%为肝硬化,62%为脓毒症,29.5%为糖尿病,29%在 ICU 死亡(中位入院时间:7.5 天)。与对照组相比,ICU 患者的基线 RBP4(25.6+/-18.4 比 43.8+/-35.0mg/L,p<0.001)和总胆固醇(TC)水平较低。存活的 ICU 患者的基线国际标准化比值(INR)的凝血酶原时间、终末期肝病模型(MELD)评分和脓毒症率较低,但估计肾小球滤过率(eGFR)和 RBP4 水平较高。eGFR、INR 和 TC 水平与 RBP4 水平独立相关。只有存活的患者在 ICU 出院后表现出 RBP4 水平的显著升高。基线 RBP4 水平和 MELD 评分分别预测 21 天(≤10mg/L)和 1 年(≥25)的死亡率。在患有基础肝脏疾病的危重症患者中,与 eGFR、INR 和 TC 水平相关,基线 RBP4 可能是短期死亡率的标志物。