Perez Elena, Bonilla Francisco A, Orange Jordan S, Ballow Mark
Allergy Associates of the Palm Beaches, North Palm Beach, FL, USA.
Boston Children's Hospital, Boston, MA, USA.
Front Immunol. 2017 May 22;8:586. doi: 10.3389/fimmu.2017.00586. eCollection 2017.
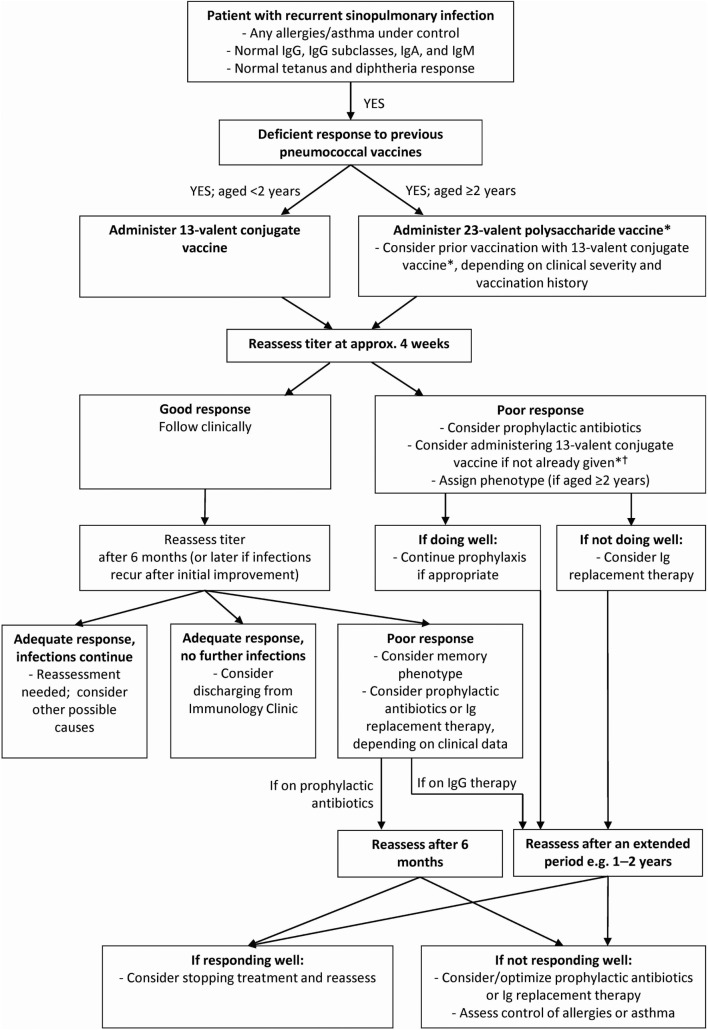
Specific antibody deficiency (SAD) is a primary immunodeficiency disease characterized by normal immunoglobulins (Igs), IgA, IgM, total IgG, and IgG subclass levels, but with recurrent infection and diminished antibody responses to polysaccharide antigens following vaccination. There is a lack of consensus regarding the diagnosis and treatment of SAD, and its clinical significance is not well understood. Here, we discuss current evidence and challenges regarding the diagnosis and treatment of SAD. SAD is normally diagnosed by determining protective titers in response to the 23-valent pneumococcal polysaccharide vaccine. However, the definition of an adequate response to immunization remains controversial, including the magnitude of response and number of pneumococcal serotypes needed to determine a normal response. Confounding these issues, anti-polysaccharide antibody responses are age- and probably serotype dependent. Therapeutic strategies and options for patients with SAD are often based on clinical experience due to the lack of focused studies and absence of a robust case definition. The mainstay of therapy for patients with SAD is antibiotic prophylaxis. However, there is no consensus regarding the frequency and severity of infections warranting antibiotic prophylaxis and no standardized regimens and no studies of efficacy. Published expert guidelines and opinions have recommended IgG therapy, which are supported by observations from retrospective studies, although definitive data are lacking. In summary, there is currently a lack of evidence regarding the efficacy of therapeutic strategies for patients with SAD. We believe that it is best to approach each patient as an individual and progress through diagnostic and therapeutic interventions together with existing practice guidelines.
特异性抗体缺陷(SAD)是一种原发性免疫缺陷疾病,其特征为免疫球蛋白(Ig)、IgA、IgM、总IgG和IgG亚类水平正常,但存在反复感染,且接种疫苗后对多糖抗原的抗体反应减弱。关于SAD的诊断和治疗缺乏共识,其临床意义也尚未得到充分理解。在此,我们讨论SAD诊断和治疗方面的现有证据及挑战。SAD通常通过检测对23价肺炎球菌多糖疫苗的保护性滴度来诊断。然而,对免疫接种充分反应的定义仍存在争议,包括反应的幅度以及确定正常反应所需的肺炎球菌血清型数量。使这些问题更加复杂的是,抗多糖抗体反应取决于年龄,可能还与血清型有关。由于缺乏针对性研究且没有明确的病例定义,SAD患者的治疗策略和选择往往基于临床经验。SAD患者治疗的主要方法是抗生素预防。然而,对于需要进行抗生素预防的感染频率和严重程度尚无共识,也没有标准化方案,且缺乏疗效研究。已发表的专家指南和意见推荐了IgG治疗,回顾性研究的观察结果支持这一推荐,尽管缺乏确凿数据。总之,目前缺乏关于SAD患者治疗策略疗效的证据。我们认为,最好将每位患者视为个体,并根据现有实践指南共同推进诊断和治疗干预措施。