Seo Won Ik, Kang Pil Moon, Yoon Jang Ho, Kim Wansuk, Chung Jae Il
Department of Urology, Busan Paik Hospital, Inje University, Busan, South Korea.
Department of Urology, Kosin University Gospel Hospital, Busan, South Korea.
Prostate Int. 2017 Jun;5(2):53-58. doi: 10.1016/j.prnil.2017.02.002. Epub 2017 Mar 3.
To evaluate the relationship between postoperative prostate-specific antigen (PSA) levels and biochemical recurrence (BCR) after radical prostatectomy, especially in patients with positive surgical margins (PSMs).
A total of 144 patients who underwent radical prostatectomies performed by a single surgeon without any neoadjuvant or adjuvant treatment were analyzed. Differences in clinicopathological factors were compared by surgical margin status, and the relationship between postoperative PSA level and BCR in patients with PSMs was evaluated.
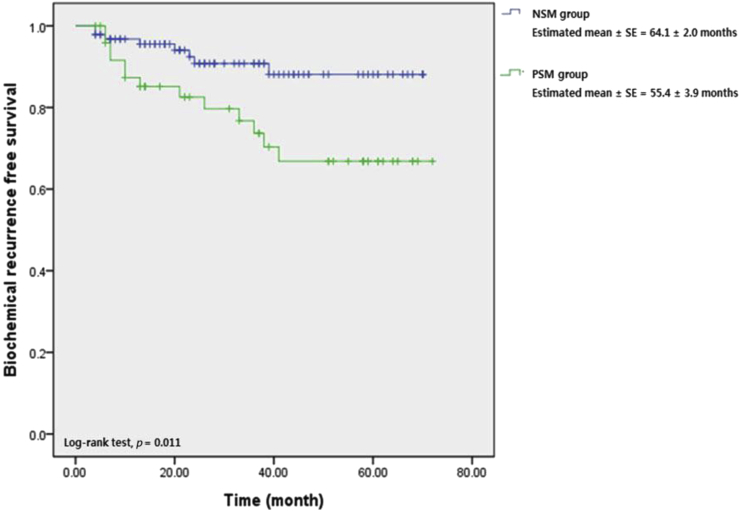
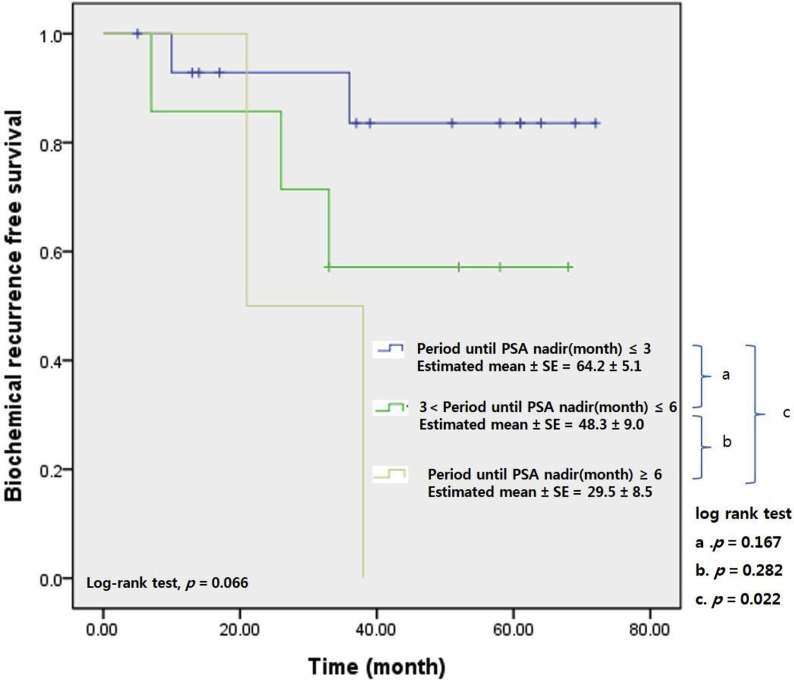
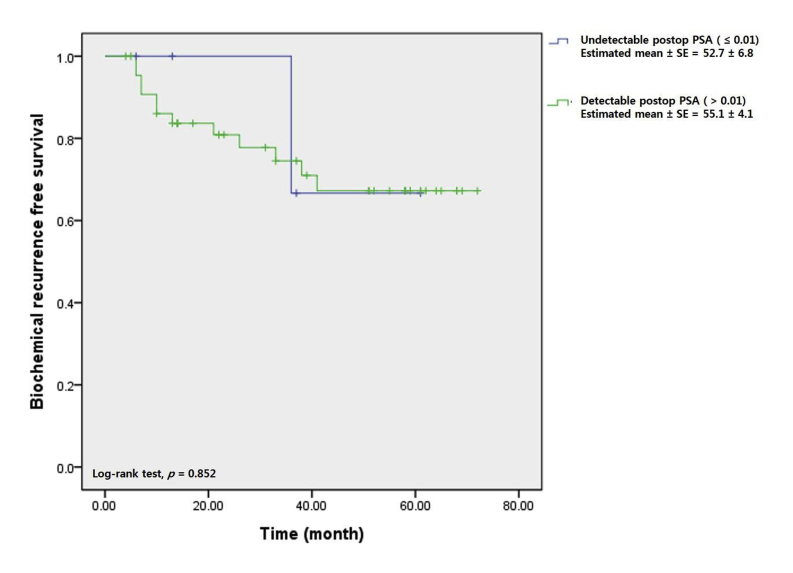
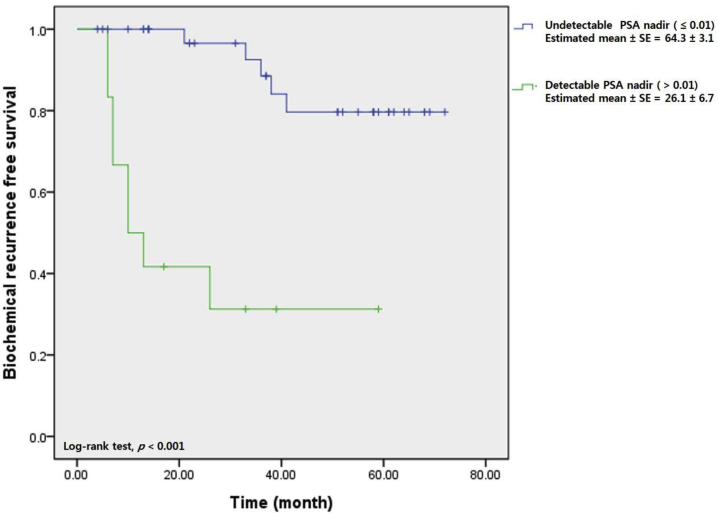
Fifty of the 144 patients (34.7%) had PSMs. Of these, 74% experienced BCR. The negative surgical margins and PSMs groups differed significantly in terms of PSA level at diagnosis, clinical T stage, and risk group by the cancer of the prostate risk assessment score ( = 0.002, = 0.002, and = 0.004, respectively). Also, the nadir PSA level, tumor volume, and BCR rate differed between the two groups ( = 0.007, = 0.015, and = 0.005, respectively) On Kaplan-Meier analysis, BCR-free survival was better in the negative surgical margins than the PSMs group (64.1 vs. 55.4 months, log-rank test, = 0.011). BCR-free survival did not differ significantly in PSMs patients according to whether PSA level was or was not detectable at 1 month postoperatively. However, BCR-free survival improved when the nadir PSA level was undetectable (compared to detectable) in PSMs patients (64.3 vs. 26.1 months, log-rank test, < 0.001). In PSMs patients belonging to the high risk group by cancer of the prostate risk assessment score, BCR-free survival was significantly better when the PSA level attained the nadir within 3 months, compared to > 6 months, postoperatively (64.2 vs. 29.5 months, log-rank test, = 0.022).
If PSA is detectable in PSMs patients until 1 month after operation, cautious observation may be possible. If the nadir is attained within 3 months postoperatively in high-risk patients with PSMs, better BCR-free survival may be expected.
评估根治性前列腺切除术后前列腺特异性抗原(PSA)水平与生化复发(BCR)之间的关系,尤其是手术切缘阳性(PSM)的患者。
分析了144例由同一外科医生进行根治性前列腺切除术且未接受任何新辅助或辅助治疗的患者。根据手术切缘状态比较临床病理因素的差异,并评估PSM患者术后PSA水平与BCR之间的关系。
144例患者中有50例(34.7%)存在PSM。其中,74%经历了BCR。手术切缘阴性和PSM组在诊断时的PSA水平、临床T分期以及前列腺癌风险评估评分的风险组方面存在显著差异(分别为P = 0.002、P = 0.002和P = 0.004)。此外,两组的PSA最低点水平、肿瘤体积和BCR率也有所不同(分别为P = 0.007、P = 0.015和P = 0.005)。在Kaplan-Meier分析中,手术切缘阴性组的无BCR生存期优于PSM组(64.1个月对55.4个月,对数秩检验,P = 0.011)。PSM患者术后1个月时PSA水平是否可检测,其无BCR生存期无显著差异。然而,PSM患者中PSA最低点水平不可检测时(与可检测相比),无BCR生存期有所改善(64.3个月对26.1个月,对数秩检验,P < 0.001)。在前列腺癌风险评估评分属于高危组的PSM患者中,术后3个月内PSA水平达到最低点时的无BCR生存期明显优于> 6个月时(64.2个月对29.5个月,对数秩检验,P = 0.022)。
如果PSM患者术后1个月内PSA可检测,可能可以进行谨慎观察。如果高危PSM患者术后3个月内达到PSA最低点,则可能预期有更好的无BCR生存期。