Sukul Devraj, Sinha Shashank S, Ryan Andrew M, Sjoding Michael W, Hummel Scott L, Nallamothu Brahmajee K
Division of Cardiovascular Medicine, Samuel and Jean Frankel Cardiovascular Center, University of Michigan, Ann Arbor.
Division of Cardiovascular Medicine, Samuel and Jean Frankel Cardiovascular Center, University of Michigan, Ann Arbor; Michigan Integrated Center for Health Analytics and Medical Prediction, Department of Internal Medicine, University of Michigan Medical School, Ann Arbor; Michigan Center for Integrative Research in Critical Care, University of Michigan, Ann Arbor; Institute for Healthcare Policy and Innovation, University of Michigan, Ann Arbor.
Am J Med. 2017 Oct;130(10):1220.e1-1220.e16. doi: 10.1016/j.amjmed.2017.05.025. Epub 2017 Jun 10.
Thirty-day readmissions among elderly Medicare patients are an important hospital quality measure. Although plans for using 30-day readmission measures are under consideration for younger patients, little is known about readmission in younger patients or the relationship between readmissions in younger and elderly patients at the same hospital.
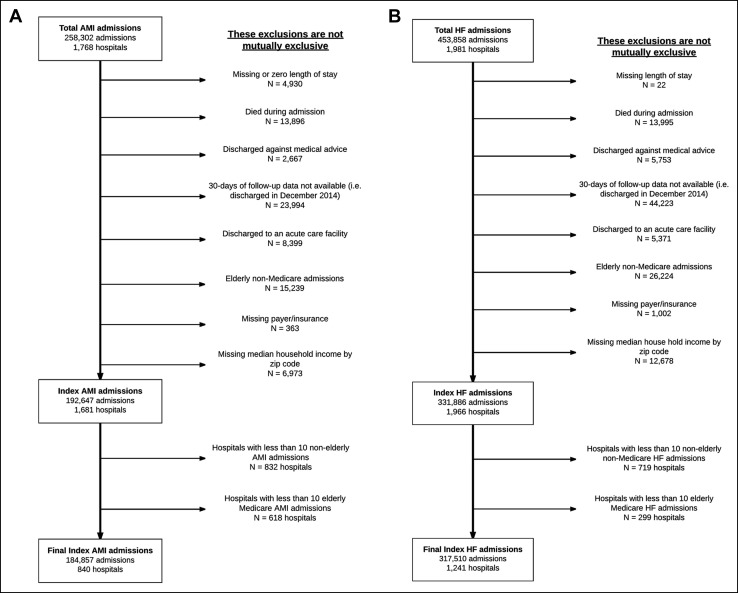
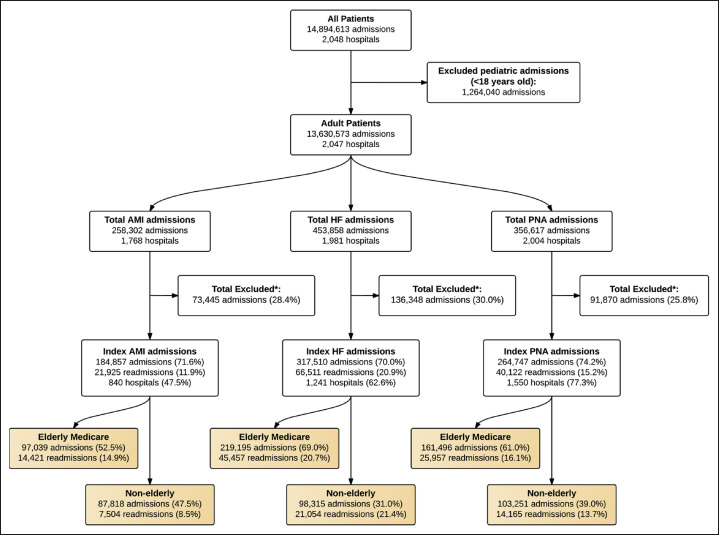
By using the 2014 Nationwide Readmissions Database, we examined readmission patterns in younger patients (18-64 years) using hierarchical models to evaluate associations between hospital 30-day, risk-standardized readmission rates in elderly Medicare patients and readmission risk in younger patients with acute myocardial infarction, heart failure, or pneumonia.
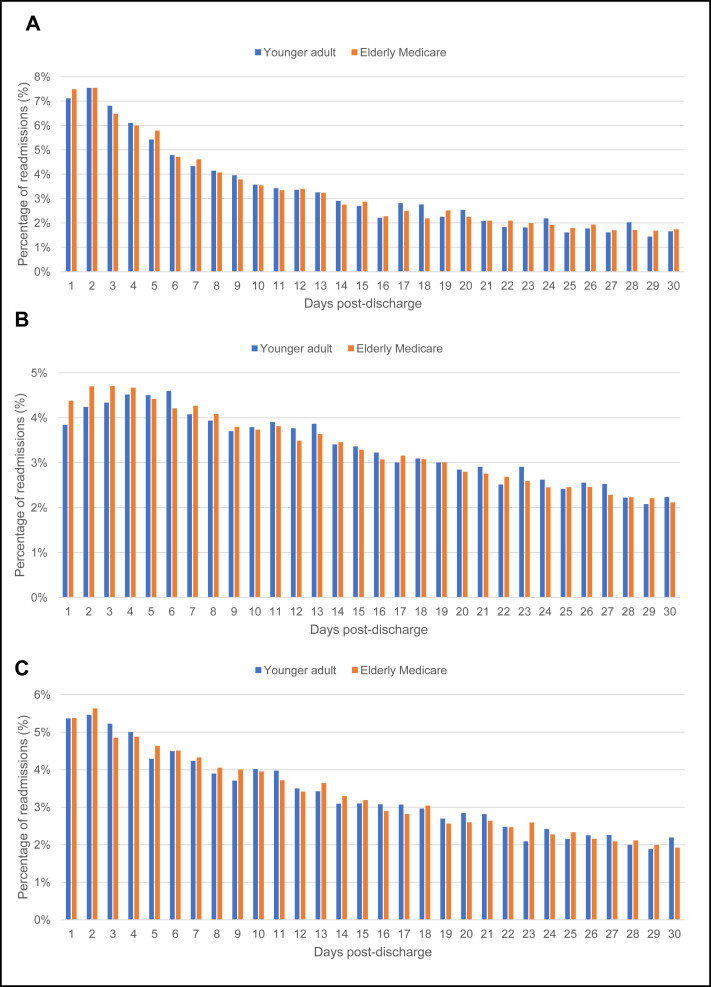
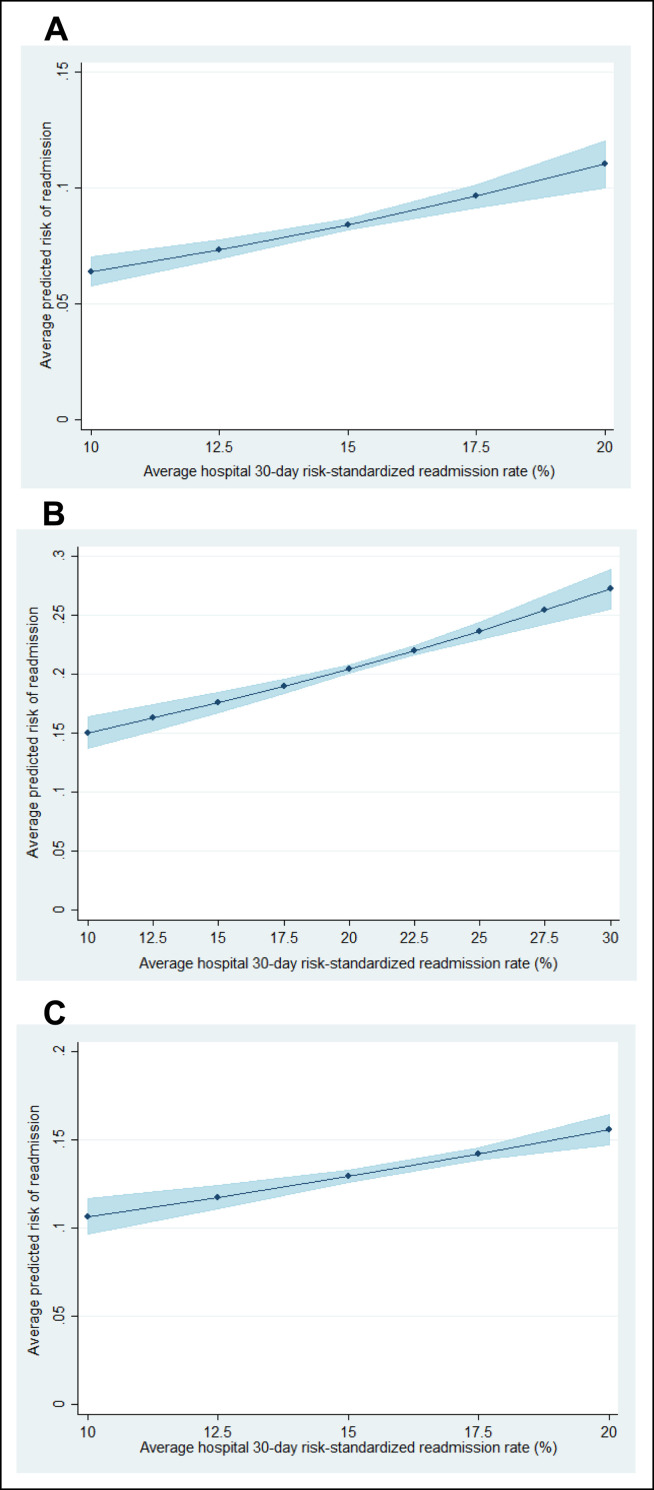
There were 87,818, 98,315, and 103,251 admissions in younger patients for acute myocardial infarction, heart failure, and pneumonia, respectively, with overall 30-day unplanned readmission rates of 8.5%, 21.4%, and 13.7%, respectively. Readmission risk in younger patients was significantly associated with hospital 30-day risk-standardized readmission rates for elderly Medicare patients for all 3 conditions. A decrease in an average hospital's 30-day, risk-standardized readmission rates from the 75th percentile to the 25th percentile was associated with reduction in younger patients' risk of readmission from 8.8% to 8.0% (difference: 0.7%; 95% confidence interval, 0.5-0.9) for acute myocardial infarction; 21.8% to 20.0% (difference: 1.8%; 95% confidence interval, 1.4-2.2) for heart failure; and 13.9% to 13.1% (difference: 0.8%; 95% confidence interval, 0.5-1.0) for pneumonia.
Among younger patients, readmission risk was moderately associated with hospital 30-day, risk-standardized readmission rates in elderly Medicare beneficiaries. Efforts to reduce readmissions among older patients may have important areas of overlap with younger patients, although further research may be necessary to identify specific mechanisms to tailor initiatives to younger patients.
老年医疗保险患者的30天再入院率是一项重要的医院质量指标。尽管针对年轻患者使用30天再入院指标的计划正在考虑之中,但对于年轻患者的再入院情况或同一家医院中年轻患者与老年患者再入院之间的关系,我们知之甚少。
通过使用2014年全国再入院数据库,我们使用分层模型研究了年轻患者(18 - 64岁)的再入院模式,以评估老年医疗保险患者的医院30天风险标准化再入院率与急性心肌梗死、心力衰竭或肺炎年轻患者再入院风险之间的关联。
年轻患者因急性心肌梗死、心力衰竭和肺炎的入院人数分别为87,818、98,315和103,251例,总体30天非计划再入院率分别为8.5%、21.4%和13.7%。对于所有这三种情况,年轻患者的再入院风险与老年医疗保险患者的医院30天风险标准化再入院率显著相关。一家医院的30天风险标准化再入院率从第75百分位数降至第25百分位数,与急性心肌梗死年轻患者的再入院风险从8.8%降至8.0%(差值:0.7%;95%置信区间,0.5 - 0.9)相关;与心力衰竭年轻患者的再入院风险从21.8%降至20.0%(差值:1.8%;95%置信区间,1.4 - 2.2)相关;与肺炎年轻患者的再入院风险从13.9%降至13.1%(差值:0.8%;95%置信区间,0.5 - 1.0)相关。
在年轻患者中,再入院风险与老年医疗保险受益人的医院30天风险标准化再入院率中度相关。降低老年患者再入院率的努力可能与年轻患者有重要的重叠领域,尽管可能需要进一步研究以确定针对年轻患者量身定制举措的具体机制。