Rhee Chanseok, Le Francois Tina, Byrd J W Thomas, Glazebrook Mark, Wong Ivan
Dalhousie University, Halifax, Nova Scotia, Canada.
Northern Ontario School of Medicine, Sudbury, Ontario, Canada.
Orthop J Sports Med. 2017 May 31;5(5):2325967117708307. doi: 10.1177/2325967117708307. eCollection 2017 May.
Femoroacetabular impingement (FAI) is a well-recognized condition that causes hip pain and can lead to early osteoarthritis if not managed properly. With the increasing awareness and efficacy of operative treatments for pincer-type FAI, there is a need for consensus on the standardized radiographic diagnosis.
To perform a systematic review of the evidence regarding imaging modalities and radiographic signs for diagnosing pincer-type FAI.
Systematic review; Level of evidence, 4.
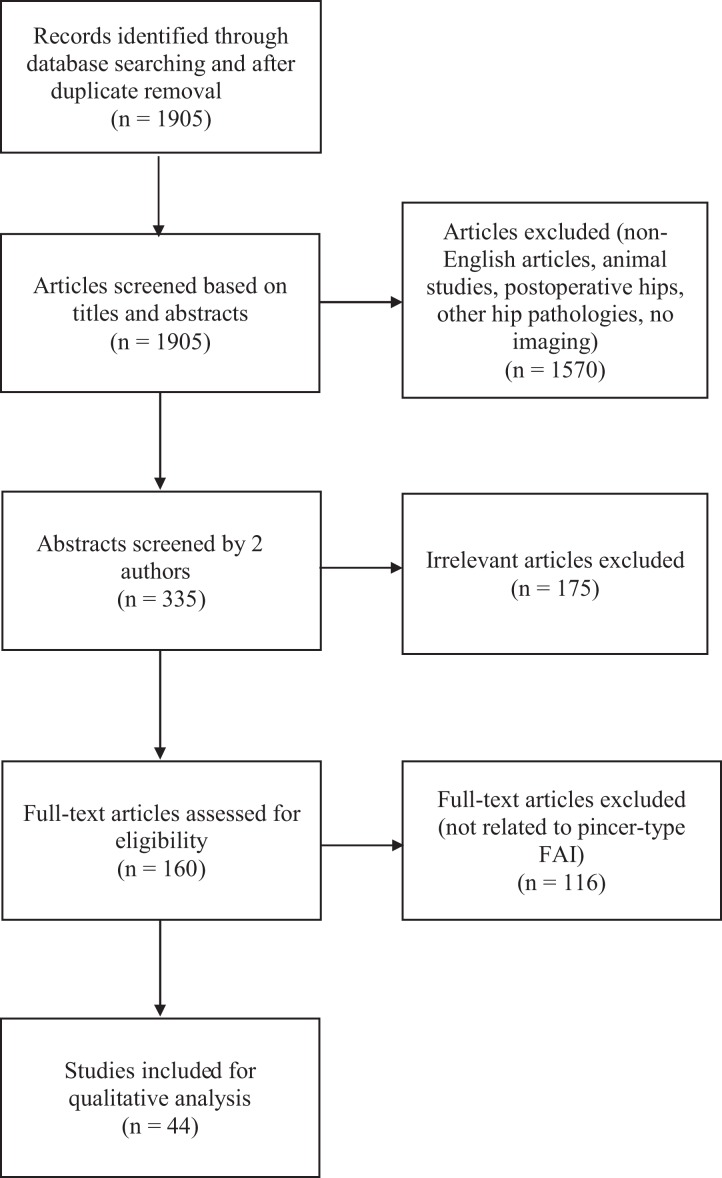
A literature review was performed in 2016 using the Cochrane, PubMed, and Embase search engines. All articles focusing on a radiographic diagnosis of pincer-type FAI were reviewed. Each of the included 44 articles was assigned the appropriate level of evidence, and the particular radiographic marker and/or type of imaging were also summarized.
There were 44 studies included in the final review. Most of the articles were level 4 evidence (26 articles), and there were 12 level 3 and 6 level 2 articles. The crossover sign was the most commonly used radiographic sign (27/44) followed by the lateral center-edge angle (22/44). Anteroposterior (AP) pelvis plain radiographs were the most commonly used imaging modality (33 studies). Poor-quality evidence exists in support of most currently used radiographic markers, including the crossover sign, lateral center-edge angle, posterior wall sign, ischial spine sign, coxa profunda, acetabular protrusion, and acetabular index. There is poor-quality conflicting evidence regarding the use of the herniation pit to diagnose pincer-type FAI. Some novel measurements, such as β-angle, acetabular roof ratio, and acetabular retroversion index, have been proposed, but they also lack support from the literature.
No strong evidence exists to support a single best set of current radiographic markers for the diagnosis of pincer-type FAI, largely due to the lack of better quality trials (levels 1 and 2) that compare conventional radiographic findings with the gold standard, which is the intraoperative findings. More sophisticated imaging modalities such as computed tomography and magnetic resonance arthrography are often needed to diagnose pincer-type FAI, and these investigations are relatively accurate in assessing labral pathology or cartilage damage.
股骨髋臼撞击症(FAI)是一种已被充分认识的疾病,可导致髋关节疼痛,若处理不当可引发早期骨关节炎。随着对钳夹型FAI手术治疗的认识不断提高且疗效显著,对标准化影像学诊断达成共识很有必要。
对有关诊断钳夹型FAI的影像学检查方法和X线征象的证据进行系统评价。
系统评价;证据等级为4级。
2016年使用Cochrane、PubMed和Embase搜索引擎进行文献综述。对所有聚焦于钳夹型FAI影像学诊断的文章进行了回顾。纳入的44篇文章分别被赋予相应的证据等级,并对特定的X线标记物和/或影像学类型进行了总结。
最终综述纳入44项研究。大多数文章为4级证据(26篇),3级证据文章有12篇,2级证据文章有6篇。交叉征是最常用的X线征象(27/44),其次是外侧中心边缘角(22/44)。前后位(AP)骨盆平片是最常用的影像学检查方法(33项研究)。支持目前大多数常用X线标记物的证据质量较差,包括交叉征、外侧中心边缘角、后壁征、坐骨棘征、髋臼深陷、髋臼突出和髋臼指数。关于使用髋臼盂唇囊肿来诊断钳夹型FAI,存在质量较差且相互矛盾的证据。一些新的测量方法,如β角、髋臼顶比率和髋臼后倾指数,已经被提出,但它们也缺乏文献支持。
目前没有强有力的证据支持一套最佳的用于诊断钳夹型FAI的X线标记物,这主要是因为缺乏将传统X线检查结果与金标准(即术中所见)进行比较的更高质量试验(1级和2级)。诊断钳夹型FAI通常需要更复杂的影像学检查方法,如计算机断层扫描和磁共振关节造影,这些检查在评估盂唇病变或软骨损伤方面相对准确。