Roth Jan A, Chrobak Carl, Schädelin Sabine, Hug Balthasar L
Division of Infectious Diseases & Hospital Epidemiology University of Basel Department of Internal Medicine Clinical Trial Unit, University Hospital Basel, Basel Department of Internal Medicine, Kantonsspital Luzern, Lucerne, Switzerland.
Medicine (Baltimore). 2017 Jun;96(24):e7155. doi: 10.1097/MD.0000000000007155.
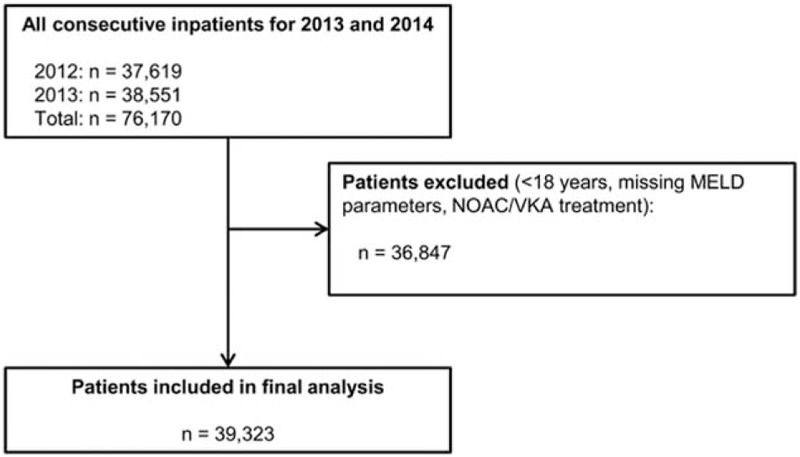
The laboratory-based model for end-stage liver disease (MELD) score reflects the function of the kidney, liver, and extrinsic coagulation pathway and might be used as a general prognostic tool for the assessment of patients. We therefore aimed to investigate a potential association of the MELD score with mortality, length of hospital stay (LOS), and disease burden in a general patient population.We performed a retrospective observational study at a tertiary referral center. From January 2012 through December 2013, all consecutive inpatients aged 18 years were eligible for the study; patients with missing MELD parameters on hospital admission and/or treatments influencing the international normalized ratio, that is, novel oral anticoagulants and vitamin K antagonists, were excluded. The MELD score on hospital admission was calculated retrospectively. The primary outcome measure was in-hospital all-cause mortality; secondary outcome measures were LOS and the number of comorbidities.A total of 39,323 inpatients were included in the final analysis. On admission, MELD scores of 15 to 19, 20 to 29, and ≥30 points (reference <15 points) showed increased hazard ratios (HRs) for in-hospital mortality in uni- and multivariable analysis with an adjusted HR of 2.52 (95% confidence interval [CI], 1.81-3.49; P < .001), 2.70 (95% CI, 1.89-3.84; P < .001), and 8.00 (95% CI, 3.91-16.39; P < .001), respectively. Increased MELD scores of 15 to 19, 20 to 29, and ≥30 points were positively associated with LOS and the number of comorbidities in uni- and multivariable analysis.In our study population consisting of adult inpatients, the MELD score on hospital admission was significantly associated with mortality, LOS, and the number of comorbidities. We suggest to prospectively validate the MELD score in inpatients as part of clinical decision support systems.
终末期肝病模型(MELD)评分反映了肾脏、肝脏和外源性凝血途径的功能,可作为评估患者的一般预后工具。因此,我们旨在研究MELD评分与普通患者群体死亡率、住院时间(LOS)和疾病负担之间的潜在关联。我们在一家三级转诊中心进行了一项回顾性观察研究。2012年1月至2013年12月,所有18岁及以上的连续住院患者均符合研究条件;入院时MELD参数缺失和/或接受影响国际标准化比值的治疗(即新型口服抗凝剂和维生素K拮抗剂)的患者被排除。入院时的MELD评分进行回顾性计算。主要结局指标是院内全因死亡率;次要结局指标是住院时间和合并症数量。最终分析共纳入39323例住院患者。入院时,MELD评分为15至19分、20至29分和≥30分(参考值<15分)在单变量和多变量分析中显示院内死亡率的风险比(HRs)增加,调整后的HR分别为2.52(95%置信区间[CI],1.81 - 3.49;P<0.001)、2.70(95%CI,1.89 - 3.84;P<0.001)和8.00(95%CI,3.91 - 16.39;P<0.001)。MELD评分增加至15至19分、20至29分和≥30分在单变量和多变量分析中与住院时间和合并症数量呈正相关。在我们由成年住院患者组成的研究群体中,入院时的MELD评分与死亡率、住院时间和合并症数量显著相关。我们建议作为临床决策支持系统的一部分,对住院患者的MELD评分进行前瞻性验证。