Cho Eunae, Jun Chung Hwan, Cho Sung Bum, Park Chang Hwan, Kim Hyun Soo, Choi Sung Kyu, Rew Jong Sun
Division of Gastroenterology, Department of Internal Medicine, Chonnam National University Medical School, Gwangju, South Korea.
Medicine (Baltimore). 2017 Jun;96(24):e7157. doi: 10.1097/MD.0000000000007157.
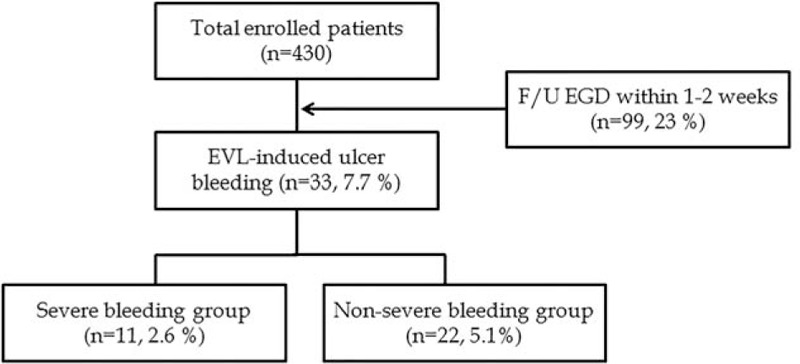
This study was aimed to determine the risk factors of endoscopic variceal ligation-(EVL) induced ulcer bleeding.The prevalence of EVL-induced ulcer bleeding is reported to be 3.6%. However, there are only limited reports of this serious complication, and the risk factors and the treatment methods are not well established.A total of 430 patients who had undergone EVL in Chonnam National University Hospital from January 2014 to October 2016 were studied. EVL was performed for prophylaxis or acute hemorrhage. The patients were classified into 2 groups: a bleeding group (n = 33) and a non-bleeding group (n = 397). The patients who had endoscopically confirmed EVL-induced ulcer bleeding were included in the bleeding group.EVL-induced ulcer bleeding occurred in 7.7% (n = 33) of the patients. In a multivariate analysis, model for end-stage liver disease (MELD) score >10 (odds ratio [OR]: 3.42, 95% confidence interval [CI]: 1.10-10.64), concomitant GV F3 (OR: 14.1, 95% CI: 2.84-71.43), and detachment of o-ring bands on follow-up endoscopy (OR: 8.06, 95% CI: 2.55-25.64) were independent predictive factors of EVL-induced ulcer bleeding. Various endoscopic modalities were attempted for hemostasis (EVL in 8 cases [24.2%], endoscopic variceal obturation [EVO] with cyanoacrylate in 6 cases [18.2%], argon plasma coagulation [APC] in 1 case (3%), Sengstaken-Blakemore (SB) tube in 3 cases [9.1%]), and proton pump inhibitor therapy only in 15 cases (45.5%).MELD score >10, concomitant GV F3, and detachment of o-ring bands on follow-up endoscopy are risk factors for EVL-induced ulcer bleeding.
本研究旨在确定内镜下静脉曲张结扎术(EVL)所致溃疡出血的危险因素。据报道,EVL所致溃疡出血的发生率为3.6%。然而,关于这种严重并发症的报道有限,其危险因素及治疗方法尚未完全明确。本研究对2014年1月至2016年10月在全南国立大学医院接受EVL治疗的430例患者进行了分析。EVL用于预防或治疗急性出血。患者被分为两组:出血组(n = 33)和非出血组(n = 397)。内镜检查确诊为EVL所致溃疡出血的患者纳入出血组。
7.7%(n = 33)的患者发生了EVL所致溃疡出血。多因素分析显示,终末期肝病模型(MELD)评分>10(比值比[OR]:3.42,95%置信区间[CI]:1.10 - 10.64)、合并胃静脉曲张F3级(OR:14.1,95% CI:2.84 - 71.43)以及随访内镜检查时o形环脱落(OR:8.06,95% CI:2.55 - 25.64)是EVL所致溃疡出血的独立预测因素。尝试了多种内镜止血方法(8例[24.2%]再次行EVL,6例[18.2%]用氰基丙烯酸酯行内镜下静脉曲张闭塞术[EVO],1例[3%]行氩离子凝固术[APC],3例[9.1%]使用三腔二囊管[SB]),仅15例(45.5%)采用质子泵抑制剂治疗。
MELD评分>10、合并胃静脉曲张F3级以及随访内镜检查时o形环脱落是EVL所致溃疡出血的危险因素。