Bukenya Dominic, Wringe Alison, Moshabela Mosa, Skovdal Morten, Ssekubugu Robert, Paparini Sara, Renju Jenny, McLean Estelle, Bonnington Oliver, Wamoyi Joyce, Seeley Janet
Medical Research Council/ Uganda Virus Research Institute, Uganda Research Unit on AIDS, Entebbe, Uganda.
Department of Epidemiology and Population Health, London School of Hygiene & Tropical Medicine, London, UK.
Sex Transm Infect. 2017 Jul;93(Suppl 3). doi: 10.1136/sextrans-2016-052970. Epub 2017 Jun 14.
To explore barriers and facilitators to accessing postdiagnosis HIV care in five sub-Saharan African countries.
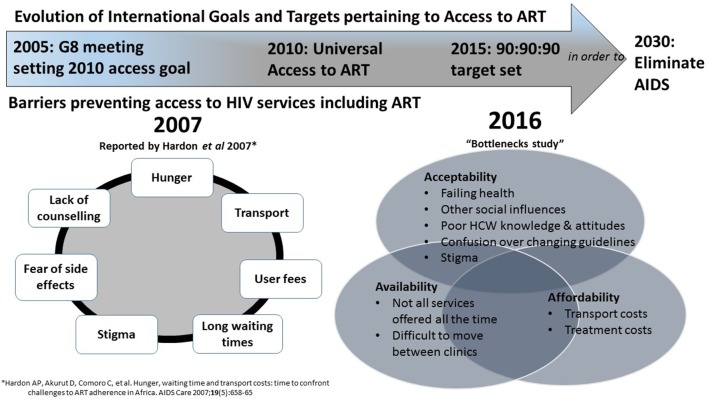
In-depth interviews were conducted with 77 people living with HIV (PLHIV) in pre-antiretroviral therapy care or not-yet-in care and 46 healthcare workers. Participants were purposely selected from health and demographic surveillance sites in Karonga (Malawi), Manicaland (Zimbabwe), uMkhanyakude (South Africa), Kisesa (Tanzania) and Rakai and Kyamulibwa (Uganda). Thematic content analysis was conducted, guided by the constructs of affordability, availability and acceptability of care.- RESULTS: Transport and treatment costs were a barrier to HIV care, although some participants travelled to distant clinics to avoid being seen by people who knew them or for specific services. Broken equipment and drug stock-outs in local clinics could also necessitate travel to other facilities. Some facilities did not offer full HIV care, or only offered all services intermittently. PLHIV who frequently travelled complained that care was seldom available to them in places they visited. Severe pain or sickness was a key driver for accessing postdiagnosis care, whereas asymptomatic PLHIV often delayed care-seeking. A belief in witchcraft was a deterrent to accessing clinical care following diagnosis. Changing antiretroviral therapy guidelines generated uncertainty among PLHIV about when to start treatment and delayed postdiagnosis care. PLHIV reported that healthcare workers' knowledge, attitudes and behaviours, and their ability to impart health education, also influenced whether they accessed HIV care.
Despite efforts to decentralise services over the past decade, many barriers to accessing HIV care persist. There is a need to increase sustained access to care for PLHIV not yet on treatment, with initiatives that encompass biomedical aspects of care alongside considerations for individual and collective challenges they faced. A failure to do so may undermine efforts to achieve universal access to antiretroviral therapy.
探讨撒哈拉以南非洲五个国家在获得艾滋病诊断后护理方面的障碍和促进因素。
对77名接受抗逆转录病毒治疗护理或尚未接受护理的艾滋病毒感染者以及46名医护人员进行了深入访谈。参与者是从卡龙加(马拉维)、马尼卡兰(津巴布韦)、乌姆卡尼亚库德(南非)、基塞萨(坦桑尼亚)以及拉凯和基亚穆利布瓦(乌干达)的健康和人口监测点中特意挑选出来的。在护理的可负担性、可获得性和可接受性等概念的指导下进行了主题内容分析。
交通和治疗费用是获得艾滋病护理的障碍,不过一些参与者前往较远的诊所,以避免被认识他们的人看到或为了获得特定服务。当地诊所设备损坏和药品缺货也可能需要前往其他机构。一些机构没有提供全面的艾滋病护理,或者只是间歇性地提供所有服务。经常出行的艾滋病毒感染者抱怨说,他们在所到之处很少能获得护理。严重疼痛或疾病是促使他们获得诊断后护理的关键因素,而无症状的艾滋病毒感染者往往推迟寻求护理。对巫术的信仰是诊断后寻求临床护理的一个阻碍因素。抗逆转录病毒治疗指南的变化使艾滋病毒感染者对何时开始治疗产生了不确定性,并推迟了诊断后护理。艾滋病毒感染者报告说,医护人员的知识、态度和行为以及他们开展健康教育的能力,也影响了他们是否能获得艾滋病护理。
尽管在过去十年中努力将服务分散化,但在获得艾滋病护理方面仍存在许多障碍。有必要通过包括护理的生物医学方面以及考虑到他们所面临的个人和集体挑战的举措,增加尚未接受治疗的艾滋病毒感染者持续获得护理的机会。否则可能会破坏实现普遍获得抗逆转录病毒治疗的努力。