Clendenning Mark, Huang Alvin, Jayasekara Harindra, Lorans Marie, Preston Susan, O'Callaghan Neil, Pope Bernard J, Macrae Finlay A, Winship Ingrid M, Milne Roger L, Giles Graham G, English Dallas R, Hopper John L, Win Aung K, Jenkins Mark A, Southey Melissa C, Rosty Christophe, Buchanan Daniel D
Colorectal Oncogenomics Group, Genetic Epidemiology Laboratory, Department of Pathology, The University of Melbourne, Parkville, VIC, 3010, Australia.
Cancer Epidemiology Centre, Cancer Council Victoria, St Kilda, VIC, 3182, Australia.
Fam Cancer. 2018 Jan;17(1):91-100. doi: 10.1007/s10689-017-0013-y.
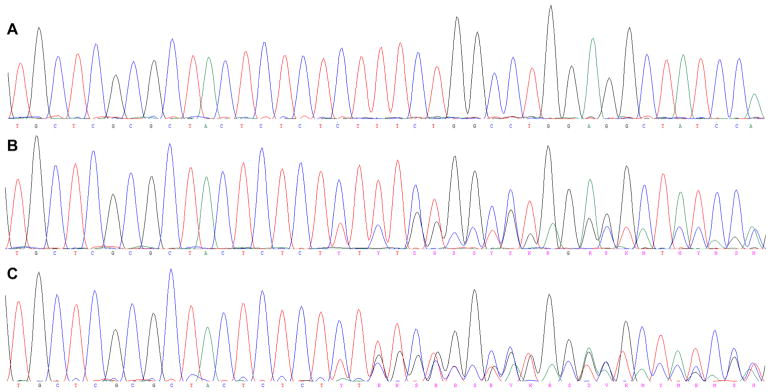
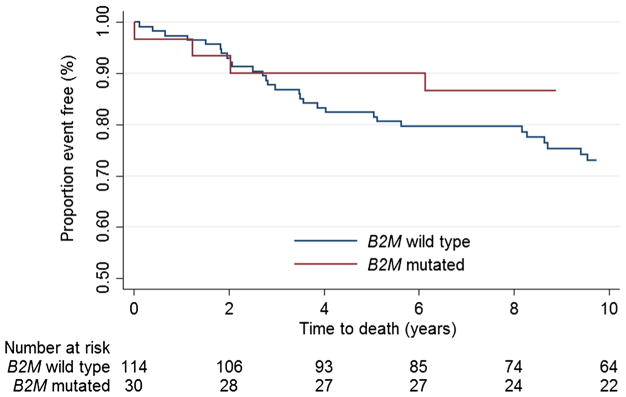
In colorectal cancers (CRCs) with tumour mismatch repair (MMR) deficiency, genes involved in the host immune response that contain microsatellites in their coding regions, including beta-2-microglobulin (B2M), can acquire mutations that may alter the immune response, tumour progression and prognosis. We screened the coding microsatellites within B2M for somatic mutations in MMR-deficient CRCs and adenomas to determine associations with tumour subtypes, clinicopathological features and survival. Incident MMR-deficient CRCs from Australasian Colorectal Cancer Family Registry (ACCFR) and the Melbourne Collaborative Cohort Study participants (n = 144) and 63 adenomas from 41 MMR gene mutation carriers from the ACCFR were screened for somatic mutations within five coding microsatellites of B2M. Hazard ratios (HR) and 95% confidence intervals (CI) for overall survival by B2M mutation status were estimated using Cox regression, adjusting for age at CRC diagnosis, sex, AJCC stage and grade. B2M mutations occurred in 30 (20.8%) of the 144 MMR-deficient CRCs (29% of the MLH1-methylated, 17% of the Lynch syndrome and 9% of the suspected Lynch CRCs). No B2M mutations were identified in the 63 adenomas tested. B2M mutations differed by site, stage, grade and lymphocytic infiltration although none reached statistical significance (p > 0.05). The HR for overall survival for B2M mutated CRC was 0.65 (95% CI 0.29-1.48) compared with B2M wild-type. We observed differences in B2M mutation status in MMR-deficient CRC by tumour subtypes, site, stage, grade, immune infiltrate and for overall survival that warrant further investigation in larger studies before B2M mutation status can be considered to have clinical utility.
在存在肿瘤错配修复(MMR)缺陷的结直肠癌(CRC)中,宿主免疫反应相关基因在其编码区域包含微卫星,其中包括β-2-微球蛋白(B2M),这些基因可能发生突变,从而改变免疫反应、肿瘤进展和预后。我们筛查了MMR缺陷型CRC和腺瘤中B2M编码微卫星的体细胞突变,以确定其与肿瘤亚型、临床病理特征和生存率的关联。对来自澳大拉西亚结直肠癌家族登记处(ACCFR)和墨尔本协作队列研究参与者的偶发性MMR缺陷型CRC(n = 144)以及来自ACCFR的41名MMR基因突变携带者的63个腺瘤,筛查B2M五个编码微卫星内的体细胞突变。使用Cox回归估计B2M突变状态的总生存率的风险比(HR)和95%置信区间(CI),并对CRC诊断时的年龄、性别、美国癌症联合委员会(AJCC)分期和分级进行校正。144例MMR缺陷型CRC中有30例(20.8%)发生B2M突变(MLH1甲基化型的29%、林奇综合征的17%、疑似林奇CRC的9%)。在检测的63个腺瘤中未发现B2M突变。B2M突变在不同位点、分期、分级和淋巴细胞浸润方面存在差异,尽管均未达到统计学意义(p > 0.05)。与B2M野生型相比,B2M突变型CRC的总生存率HR为0.65(95% CI 0.29 - 1.48)。我们观察到MMR缺陷型CRC中B2M突变状态在肿瘤亚型、位点、分期、分级、免疫浸润以及总生存率方面存在差异,在B2M突变状态被认为具有临床实用性之前,需要在更大规模的研究中进行进一步调查。