Buchanan Daniel D, Clendenning Mark, Rosty Christophe, Eriksen Stine V, Walsh Michael D, Walters Rhiannon J, Thibodeau Stephen N, Stewart Jenna, Preston Susan, Win Aung Ko, Flander Louisa, Ouakrim Driss Ait, Macrae Finlay A, Boussioutas Alex, Winship Ingrid M, Giles Graham G, Hopper John L, Southey Melissa C, English Dallas, Jenkins Mark A
Colorectal Oncogenomics Group, Genetic Epidemiology Laboratory, Department of Pathology, The University of Melbourne, Parkville, Victoria, Australia.
Centre for Epidemiology and Biostatistics, Melbourne School of Population and Global Health, The University of Melbourne, Parkville, Victoria, Australia.
J Gastroenterol Hepatol. 2017 Feb;32(2):427-438. doi: 10.1111/jgh.13468.
Tumor testing of colorectal cancers (CRC) for mismatch repair (MMR) deficiency is an effective approach to identify carriers of germline MMR gene mutation (Lynch syndrome). The aim of this study was to identify MMR gene mutation carriers in two cohorts of population-based CRC utilizing a combination of tumor and germline testing approaches.
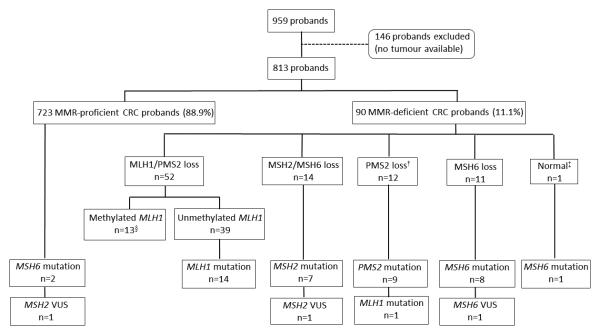
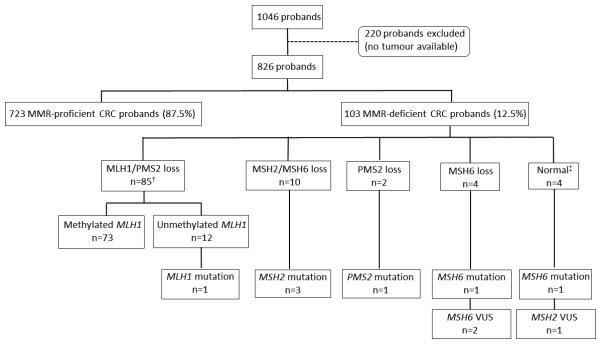
Colorectal cancers from 813 patients diagnosed with CRC < 60 years of age from the Australasian Colorectal Cancer Family Registry (ACCFR) and from 826 patients from the Melbourne Collaborative Cohort Study (MCCS) were tested for MMR protein expression using immunohistochemistry, microsatellite instability (MSI), BRAF somatic mutation, and for MLH1 methylation. MMR gene mutation testing (Sanger sequencing and Multiplex Ligation Dependent Probe Amplification) was performed on germline DNA of patients with MMR-deficient tumors and a subset of MMR-proficient CRCs.
Of the 813 ACCFR probands, 90 probands demonstrated tumor MMR deficiency (11.1%), and 42 had a MMR gene germline mutation (5.2%). For the MCCS, MMR deficiency was identified in the tumors of 103 probands (12.5%) and seven had a germline mutation (0.8%). All the mutation carriers were diagnosed prior to 70 years of age. Probands with a MMR-deficient CRC without MLH1 methylation and a gene mutation were considered Lynch-like and comprised 41.1% and 25.2% of the MMR-deficient CRCs for the ACCFR and MCCS, respectively.
Identification of MMR gene mutation carriers in Australian CRC-affected patients is optimized by immunohistochemistry screening of CRC diagnosed before 70 years of age. A significant proportion of MMR-deficient CRCs will have unknown etiology (Lynch-like) proving problematic for clinical management.
对结直肠癌(CRC)进行错配修复(MMR)缺陷的肿瘤检测是识别种系MMR基因突变携带者(林奇综合征)的有效方法。本研究的目的是通过结合肿瘤和种系检测方法,在两个基于人群的CRC队列中识别MMR基因突变携带者。
对来自澳大利亚结直肠癌家族登记处(ACCFR)的813例年龄<60岁的CRC患者以及墨尔本协作队列研究(MCCS)的826例患者的结直肠癌进行MMR蛋白表达检测,采用免疫组织化学、微卫星不稳定性(MSI)、BRAF体细胞突变检测以及MLH1甲基化检测。对MMR缺陷肿瘤患者和一部分MMR功能正常的CRC患者的种系DNA进行MMR基因突变检测(桑格测序和多重连接依赖探针扩增)。
在813例ACCFR先证者中,90例先证者表现出肿瘤MMR缺陷(11.1%),42例有MMR基因种系突变(5.2%)。对于MCCS,在103例先证者(12.5%)的肿瘤中发现了MMR缺陷,7例有生殖系突变(0.8%)。所有突变携带者均在70岁之前被诊断。没有MLH1甲基化和基因突变的MMR缺陷CRC先证者被认为是林奇样病例,分别占ACCFR和MCCS中MMR缺陷CRC的41.1%和25.2%。
通过对70岁之前诊断的CRC进行免疫组织化学筛查,可优化对澳大利亚CRC患者中MMR基因突变携带者的识别。相当一部分MMR缺陷的CRC病因不明(林奇样),这给临床管理带来了问题。