Li Linxin, Geraghty Olivia C, Mehta Ziyah, Rothwell Peter M
Centre for Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, John Radcliffe Hospital, University of Oxford, Oxford, UK.
Centre for Prevention of Stroke and Dementia, Nuffield Department of Clinical Neurosciences, John Radcliffe Hospital, University of Oxford, Oxford, UK.
Lancet. 2017 Jul 29;390(10093):490-499. doi: 10.1016/S0140-6736(17)30770-5. Epub 2017 Jun 13.
Lifelong antiplatelet treatment is recommended after ischaemic vascular events, on the basis of trials done mainly in patients younger than 75 years. Upper gastrointestinal bleeding is a serious complication, but had low case fatality in trials of aspirin and is not generally thought to cause long-term disability. Consequently, although co-prescription of proton-pump inhibitors (PPIs) reduces upper gastrointestinal bleeds by 70-90%, uptake is low and guidelines are conflicting. We aimed to assess the risk, time course, and outcomes of bleeding on antiplatelet treatment for secondary prevention in patients of all ages.
We did a prospective population-based cohort study in patients with a first transient ischaemic attack, ischaemic stroke, or myocardial infarction treated with antiplatelet drugs (mainly aspirin based, without routine PPI use) after the event in the Oxford Vascular Study from 2002 to 2012, with follow-up until 2013. We determined type, severity, outcome (disability or death), and time course of bleeding requiring medical attention by face-to-face follow-up for 10 years. We estimated age-specific numbers needed to treat (NNT) to prevent upper gastrointestinal bleeding with routine PPI co-prescription on the basis of Kaplan-Meier risk estimates and relative risk reduction estimates from previous trials.
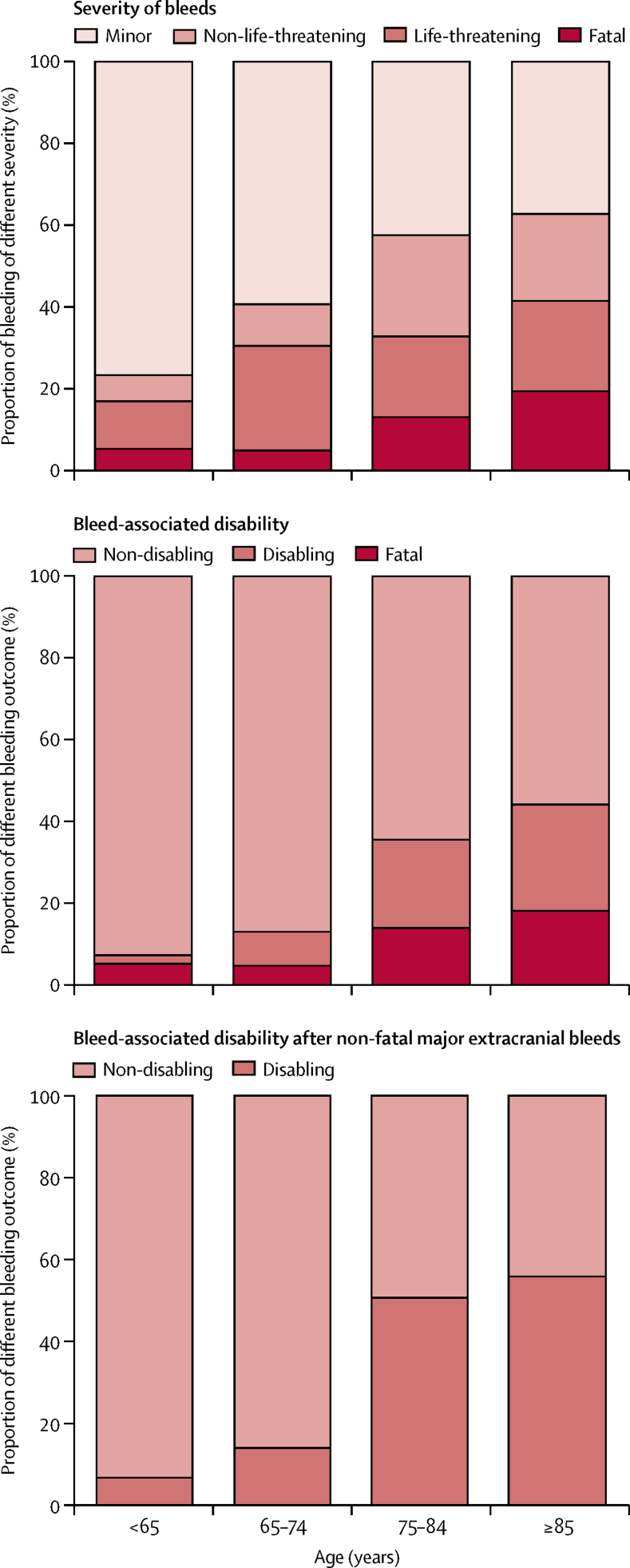
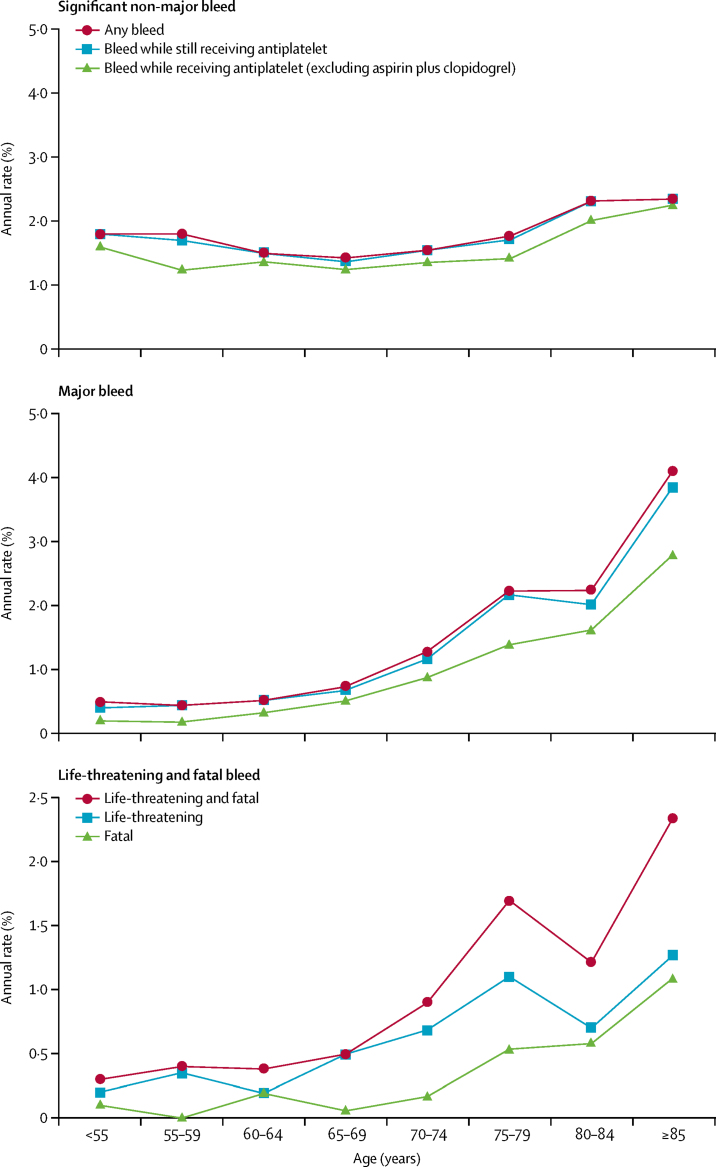
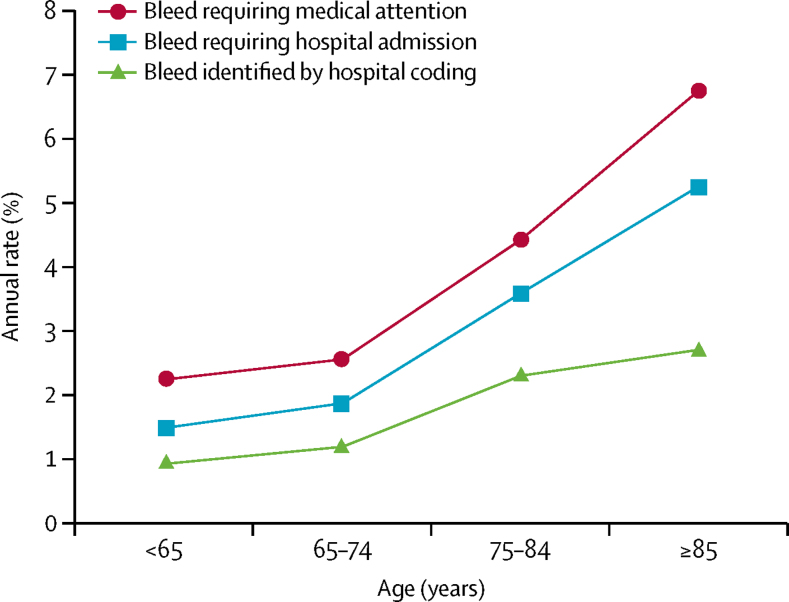
3166 patients (1582 [50%] aged ≥75 years) had 405 first bleeding events (n=218 gastrointestinal, n=45 intracranial, and n=142 other) during 13 509 patient-years of follow-up. Of the 314 patients (78%) with bleeds admitted to hospital, 117 (37%) were missed by administrative coding. Risk of non-major bleeding was unrelated to age, but major bleeding increased steeply with age (≥75 years hazard ratio [HR] 3·10, 95% CI 2·27-4·24; p<0·0001), particularly for fatal bleeds (5·53, 2·65-11·54; p<0·0001), and was sustained during long-term follow-up. The same was true of major upper gastrointestinal bleeds (≥75 years HR 4·13, 2·60-6·57; p<0·0001), particularly if disabling or fatal (10·26, 4·37-24·13; p<0·0001). At age 75 years or older, major upper gastrointestinal bleeds were mostly disabling or fatal (45 [62%] of 73 patients vs 101 [47%] of 213 patients with recurrent ischaemic stroke), and outnumbered disabling or fatal intracerebral haemorrhage (n=45 vs n=18), with an absolute risk of 9·15 (95% CI 6·67-12·24) per 1000 patient-years. The estimated NNT for routine PPI use to prevent one disabling or fatal upper gastrointestinal bleed over 5 years fell from 338 for individuals younger than 65 years, to 25 for individuals aged 85 years or older.
In patients receiving aspirin-based antiplatelet treatment without routine PPI use, the long-term risk of major bleeding is higher and more sustained in older patients in practice than in the younger patients in previous trials, with a substantial risk of disabling or fatal upper gastrointestinal bleeding. Given that half of the major bleeds in patients aged 75 years or older were upper gastrointestinal, the estimated NNT for routine PPI use to prevent such bleeds is low, and co-prescription should be encouraged.
Wellcome Trust, Wolfson Foundation, British Heart Foundation, Dunhill Medical Trust, National Institute of Health Research (NIHR), and the NIHR Oxford Biomedical Research Centre.
基于主要在75岁以下患者中进行的试验,缺血性血管事件后推荐终身抗血小板治疗。上消化道出血是一种严重并发症,但在阿司匹林试验中的病死率较低,一般认为不会导致长期残疾。因此,尽管联合使用质子泵抑制剂(PPI)可使上消化道出血减少70% - 90%,但其使用率较低且指南存在冲突。我们旨在评估各年龄段患者二级预防抗血小板治疗中出血的风险、时间进程及结局。
我们在牛津血管研究中对2002年至2012年发生首次短暂性脑缺血发作、缺血性卒中或心肌梗死并在事件后接受抗血小板药物治疗(主要基于阿司匹林,未常规使用PPI)的患者进行了一项基于人群的前瞻性队列研究,随访至2013年。我们通过10年的面对面随访确定了需要医疗关注的出血类型、严重程度、结局(残疾或死亡)及时间进程。我们根据Kaplan - Meier风险估计和既往试验的相对风险降低估计值,估算了常规联合使用PPI预防上消化道出血的年龄特异性治疗所需人数(NNT)。
3166例患者(1582例[50%]年龄≥75岁)在13509患者年的随访期间发生了405次首次出血事件(218例为胃肠道出血,45例为颅内出血,142例为其他出血)。在314例(78%)因出血住院的患者中,行政编码遗漏了117例(37%)。非大出血风险与年龄无关,但大出血风险随年龄急剧增加(≥75岁风险比[HR] 3.10,95%可信区间[CI] 2.27 - 4.24;p < 0.0001),尤其是致命性出血(5.53,2.65 - 11.54;p < 0.0001),且在长期随访中持续存在。重大上消化道出血情况相同(≥75岁HR 4.13,2.60 - 6.57;p < 0.0001),尤其是致残或致命性出血(10.26,4.37 - 24.13;p < 0.0001)。在75岁及以上患者中,重大上消化道出血大多导致残疾或死亡(73例患者中的45例[62%],而复发性缺血性卒中患者213例中的101例[47%]),且超过致残或致命性脑出血(45例对18例),每1000患者年的绝对风险为9.15(95% CI 6.67 - 12.24)。5年内常规使用PPI预防一次致残或致命性上消化道出血的估计NNT从65岁以下个体的338降至85岁及以上个体的25。
在未常规使用PPI的基于阿司匹林的抗血小板治疗患者中,实际老年患者的大出血长期风险高于既往试验中的年轻患者且持续时间更长,存在显著的致残或致命性上消化道出血风险。鉴于75岁及以上患者中一半的大出血为上消化道出血,常规使用PPI预防此类出血的估计NNT较低,应鼓励联合用药。
惠康信托基金会、沃尔夫森基金会、英国心脏基金会、邓希尔医学信托基金、国家卫生研究院(NIHR)以及NIHR牛津生物医学研究中心。