Harris Jeremy P, Patel Manali I, Loo Billy W, Wakelee Heather A, Diehn Maximilian
Department of Radiation Oncology, Stanford University School of Medicine, 875 Blake Wilbur Dr, MC 5847, Stanford, CA 94305, United States.
Division of Oncology, Department of Medicine, Stanford University School of Medicine, 269 Campus Dr, Stanford, CA 94305, United States.
Lung Cancer. 2017 Jun;108:173-182. doi: 10.1016/j.lungcan.2017.03.017. Epub 2017 Mar 29.
In patients receiving concurrent chemoradiation for locally advanced non-small cell lung cancer (NSCLC), consolidation chemotherapy is frequently given even though several randomized trials have failed to show a benefit. We explored the potential benefits of consolidation chemotherapy using a population-based comparative effectiveness approach.
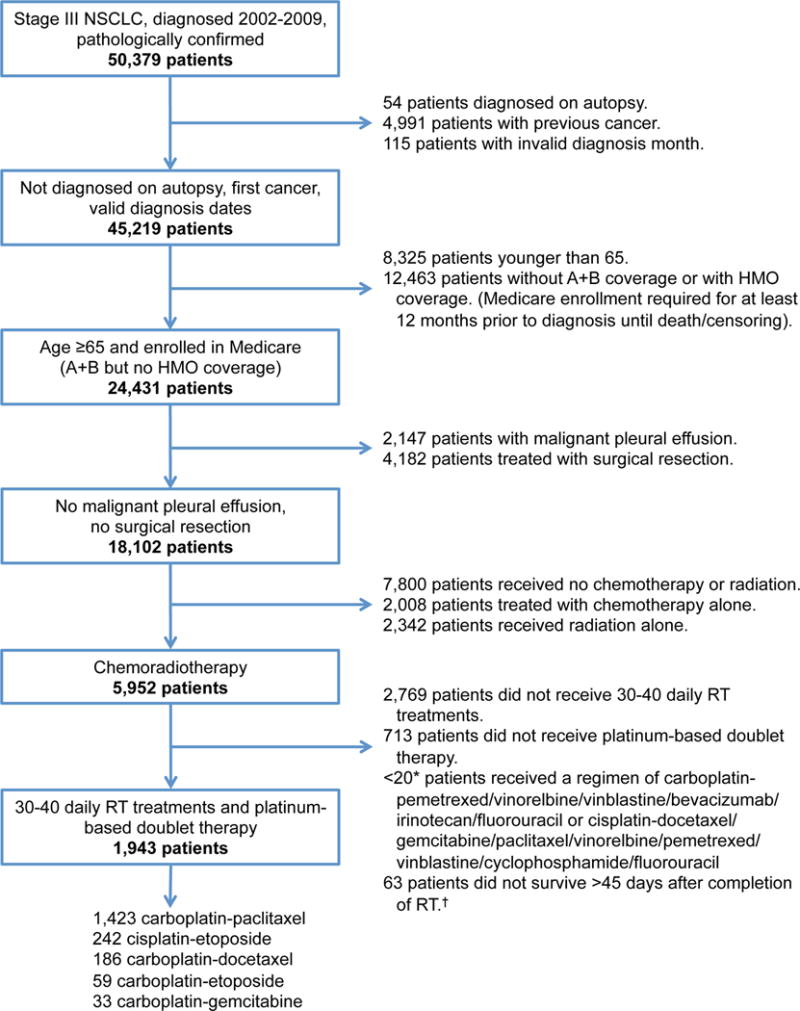
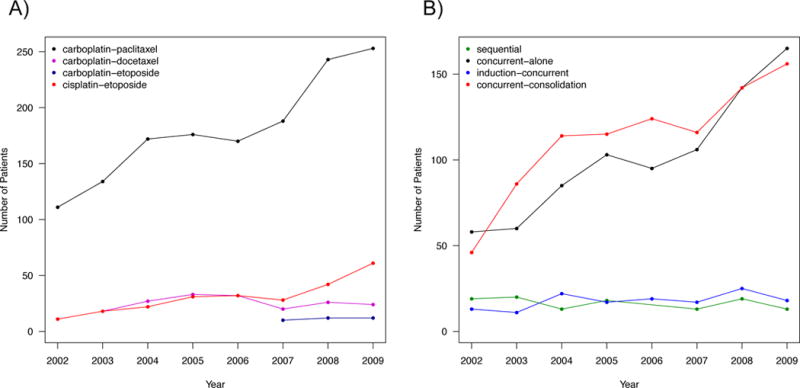
Surveillance, Epidemiology, and End Results-Medicare was used to identify patients with Stage III NSCLC aged ≥65 and diagnosed 2002-2009. We selected patients who received concurrent chemoradiotherapy and determined whether they were (concurrent-consolidation) or were not (concurrent-alone) treated with consolidation chemotherapy. Outcomes were overall and cancer specific survival using a conditional landmark analysis approach.
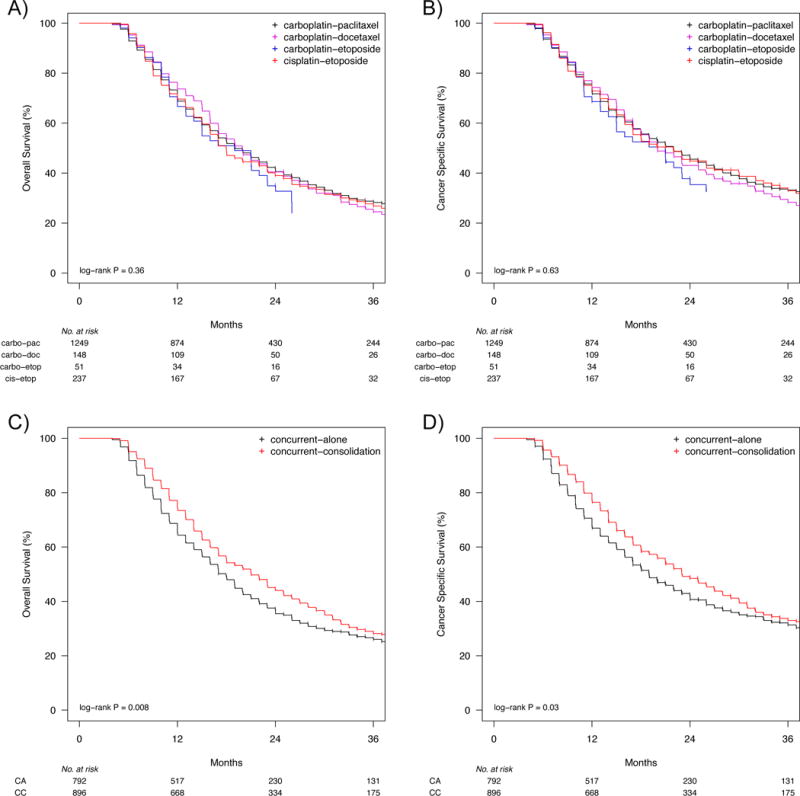
1688 patients treated with concurrent-alone or concurrent-consolidation were identified with a median follow up of 29 months. Choice of chemotherapy agents did not correlate with outcome. For concurrent-consolidation versus concurrent-alone, the median overall survival was 21 months versus 18 months, respectively (log-rank p=0.008) and the median cancer specific survival was 23 months versus 19 months, respectively (log-rank p=0.03). On multivariate analysis, concurrent-consolidation remained associated with improved overall survival (HR 0.85, p=0.04), and there was a trend for improved cancer specific survival (HR 0.87, p=0.12). Inverse probability of treatment weighting using propensity scores demonstrated similar findings. Importantly, the benefit of concurrent-consolidation held only for patients treated with carboplatin-taxane but not with cisplatin-etoposide.
Survival outcomes were similar among the five most commonly employed platinum-based doublets. We found that patients receiving cisplatin during radiation do not appear to benefit from additional chemotherapy. However, for patients receiving carboplatin, consolidation chemotherapy was associated with improved overall and cancer specific survival.
在接受同步放化疗的局部晚期非小细胞肺癌(NSCLC)患者中,尽管多项随机试验未能显示出巩固化疗的益处,但仍经常给予巩固化疗。我们采用基于人群的比较有效性方法探讨了巩固化疗的潜在益处。
利用监测、流行病学和最终结果-医疗保险数据库识别2002年至2009年诊断为III期NSCLC且年龄≥65岁的患者。我们选择接受同步放化疗的患者,并确定他们是否接受了巩固化疗(同步-巩固组)或未接受巩固化疗(单纯同步组)。使用条件性地标分析方法评估总生存期和癌症特异性生存期。
共识别出1688例接受单纯同步或同步-巩固治疗的患者,中位随访时间为29个月。化疗药物的选择与预后无关。与单纯同步组相比,同步-巩固组的中位总生存期分别为21个月和18个月(对数秩检验p=0.008),中位癌症特异性生存期分别为23个月和19个月(对数秩检验p=0.03)。多因素分析显示,同步-巩固治疗仍与总生存期改善相关(风险比0.85,p=0.04),癌症特异性生存期有改善趋势(风险比0.87,p=0.12)。使用倾向评分的治疗加权逆概率显示了类似的结果。重要的是,同步-巩固治疗的益处仅适用于接受卡铂-紫杉烷治疗的患者,而不适用于接受顺铂-依托泊苷治疗的患者。
五种最常用的铂类双联化疗方案的生存结果相似。我们发现,放疗期间接受顺铂治疗的患者似乎无法从额外的化疗中获益。然而,对于接受卡铂治疗的患者,巩固化疗与总生存期和癌症特异性生存期的改善相关。