Raschke Michael J, Kittl Christoph, Domnick Christoph
Department of Trauma, Hand and Reconstructive Surgery, Westphaelian Wilhelms University Muenster, Waldeyer Strasse 1, 48149 Muenster, Germany.
EFORT Open Rev. 2017 May 11;2(5):241-249. doi: 10.1302/2058-5241.2.160067. eCollection 2017 May.
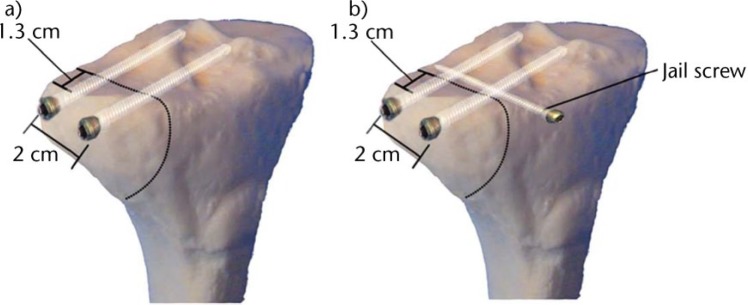
Partial tibial plateau fractures may occur as a consequence of either valgus or varus trauma combined with a rotational and axial compression component.High-energy trauma may result in a more complex and multi-fragmented fracture pattern, which occurs predominantly in young people. Conversely, a low-energy mechanism may lead to a pure depression fracture in the older population with weaker bone density.Pre-operative classification of these fractures, by Müller AO, Schatzker or novel CT-based methods, helps to understand the fracture pattern and choose the surgical approach and treatment strategy in accordance with estimated bone mineral density and the individual history of each patient.Non-operative treatment may be considered for non-displaced intra-articular fractures of the lateral tibial condyle. Intra-articular joint displacement ⩾ 2 mm, open fractures or fractures of the medial condyle should be reduced and fixed operatively. Autologous, allogenic and synthetic bone substitutes can be used to fill bone defects.A variety of minimally invasive approaches, temporary osteotomies and novel techniques (e.g. arthroscopically assisted reduction or 'jail-type' screw osteosynthesis) offer a range of choices for the individual and are potentially less invasive treatments.Rehabilitation protocols should be carefully planned according to the degree of stability achieved by internal fixation, bone mineral density and other patient-specific factors (age, compliance, mobility). To avoid stiffness, early functional mobilisation plays a major role in rehabilitation. In the elderly, low-energy trauma and impression fractures are indicators for the further screening and treatment of osteoporosis. Cite this article: 2017;2. DOI: 10.1302/2058-5241.2.160067. Originally published online at www.efortopenreviews.org.
部分胫骨平台骨折可能由外翻或内翻创伤合并旋转和轴向压缩成分引起。高能量创伤可能导致更复杂的多碎片骨折模式,主要发生在年轻人中。相反,低能量机制可能导致老年人群中骨密度较弱的单纯凹陷骨折。通过Müller AO、Schatzker或基于CT的新方法对这些骨折进行术前分类,有助于了解骨折模式,并根据估计的骨矿物质密度和每位患者的个体病史选择手术入路和治疗策略。对于外侧胫骨髁无移位的关节内骨折,可考虑非手术治疗。关节内移位≥2 mm、开放性骨折或内侧髁骨折应进行手术复位和固定。自体、异体和合成骨替代物可用于填充骨缺损。多种微创入路、临时截骨术和新技术(如关节镜辅助复位或“监狱型”螺钉接骨术)为个体提供了一系列选择,且可能是侵入性较小的治疗方法。康复方案应根据内固定所达到的稳定程度、骨矿物质密度和其他患者特定因素(年龄、依从性、活动能力)仔细规划。为避免僵硬,早期功能活动在康复中起主要作用。在老年人中,低能量创伤和凹陷骨折是进一步筛查和治疗骨质疏松症的指标。引用本文:2017;2。DOI:10.1302/2058-5241.2.160067。最初在线发表于www.efortopenreviews.org。