Department of Gyaecology, Section Minimally Invasive Surgery, Leiden University Medical Centre, PO Box 9600, 2300 RC, Leiden, The Netherlands.
Department of Gynecology, Academic Medical Centre, Amsterdam, The Netherlands.
Surg Endosc. 2017 Dec;31(12):5418-5426. doi: 10.1007/s00464-017-5624-8. Epub 2017 Jun 20.
The success of newly introduced surgical techniques is generally primarily assessed by surgical outcome measures. However, data on medical liability should concomitantly be used to evaluate provided care as they give a unique insight into substandard care from patient's point of view. The aim of this study was to analyze the number and type of medical claims after laparoscopic gynecologic procedures since the introduction of advanced laparoscopy two decades ago. Secondly, our objective was to identify trends and/or risk factors associated with these claims.
To identify the claims, we searched the databases of the two largest medical liability mutual insurance companies in The Netherlands (MediRisk and Centramed), covering together 96% of the Dutch hospitals. All claims related to laparoscopic gynecologic surgery and filed between 1993 and 2015 were included.
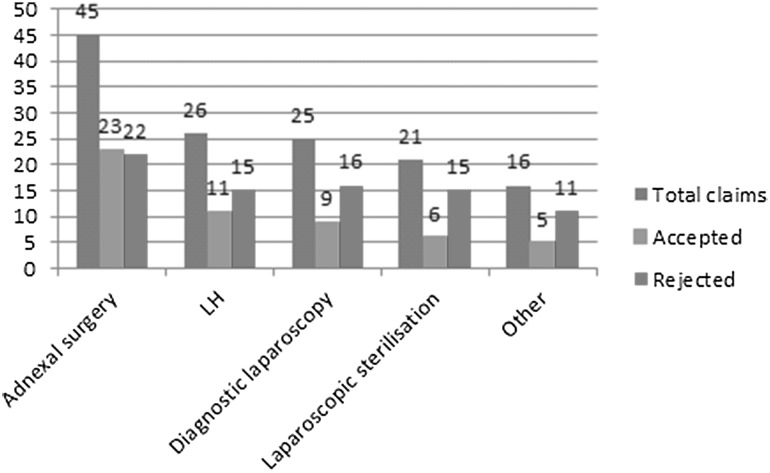
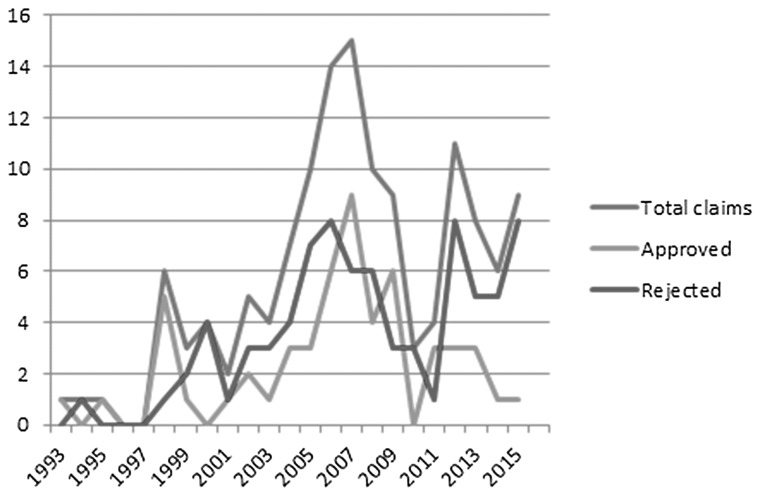
A total of 133 claims met our inclusion criteria, of which 54 were accepted claims (41%) and 79 rejected (59%). The number of claims remained relatively constant over time. The majority of claims were filed for visceral and/or vascular injuries (82%), specifically to the bowel (40%) and ureters (20%). More than one-third of the injuries were entry related (38%) and 77% of the claims were filed after non-advanced procedures. A delay in diagnosing injuries was the primary reason for financial compensation (33%). The median sum paid to patients was €12,000 (500-848,689). In 90 claims, an attorney was defending the patient (83% for the accepted claims; 57% for the rejected claims).
The number of claims remained relatively constant during the study period. Most claims were provoked by bowel and ureter injuries. Delay in recognizing injuries was the most encountered reason for granting financial compensation. Entering the abdominal cavity during laparoscopy continues to be a potential dangerous step. As a result, gynecologists are recommended to thoroughly counsel patients undergoing any laparoscopic procedure, even regarding the risk of entry-related injuries.
新引入的外科技术的成功通常主要通过手术结果来评估。然而,同时应该使用医疗责任数据来评估所提供的护理,因为它们从患者的角度提供了对护理标准不足的独特见解。本研究的目的是分析自二十年前先进腹腔镜技术引入以来腹腔镜妇科手术后的医疗索赔数量和类型。其次,我们的目标是确定与这些索赔相关的趋势和/或风险因素。
为了识别这些索赔,我们在荷兰两家最大的医疗责任相互保险公司(MediRisk 和 Centramed)的数据库中进行了搜索,这两家公司涵盖了荷兰 96%的医院。所有与腹腔镜妇科手术相关并在 1993 年至 2015 年期间提交的索赔均包括在内。
共有 133 项索赔符合我们的纳入标准,其中 54 项被接受(41%),79 项被拒绝(59%)。索赔数量随时间相对保持稳定。大多数索赔是针对内脏和/或血管损伤提出的(82%),特别是对肠道(40%)和输尿管(20%)。超过三分之一的损伤与进入相关(38%),77%的索赔是在非先进程序后提出的。诊断损伤的延迟是获得经济赔偿的主要原因(33%)。支付给患者的中位数金额为 12,000 欧元(500-848,689 欧元)。在 90 项索赔中,有一名律师为患者辩护(接受索赔的占 83%;拒绝索赔的占 57%)。
在研究期间,索赔数量相对保持稳定。大多数索赔是由肠道和输尿管损伤引起的。识别损伤的延迟是获得经济赔偿的最常见原因。在腹腔镜检查期间进入腹腔仍然是一个潜在的危险步骤。因此,建议妇科医生对接受任何腹腔镜手术的患者进行彻底咨询,甚至包括与进入相关的损伤风险。